Levitra enthält Vardenafil, das eine kürzere Wirkdauer als Tadalafil hat, dafür aber schnell einsetzt. Männer, die diskret bestellen möchten, suchen häufig nach levitra kaufen ohne rezept. Dabei spielt die rechtliche Lage in der Schweiz eine wichtige Rolle.
Anomalous self-experience and childhood trauma in first-episode schizophrenia

Available online at
Anomalous self-experience and childhood trauma in
Elisabeth Hauga,⁎, Merete Øiea,b, Ole A. Andreassen c, Unni Bratlien a, Barnaby Nelson d,
Monica Aas c, Paul Møller e, Ingrid Melle c
aDivision of Mental Health, Innlandet Hospital Trust, Ottestad, Norway
bDepartment of Psychology, University of Oslo, Oslo, Norway
cNORMENT, KG Jebsen Centre for Psychosis Research, Institute of Clinical Medicine, Division of Mental Health and Addiction, University of Oslo, and Oslo
University Hospital, Oslo, Norway
dOrygen Youth Health Research Centre, Centre for Youth Mental Health, University of Melbourne, Melbourne, Australia
eDepartment of Mental Health Research and Development, Division of Mental Health and Addiction, Vestre Viken Hospital Trust, Drammen, Norway
Background: Anomalous self-experiences (ASEs) are viewed as core features of schizophrenia. Childhood trauma (CT) has been postulatedas a risk factor for developing schizophrenia.
Aim: The aim of this study is to investigate the relationships between CT, depression and ASEs in schizophrenia.
Method: ASEs were assessed in 55 patients in the early treated phases of schizophrenia using the Examination of Anomalous Self-Experience (EASE) instrument. Data on CT were collected using the Childhood Trauma Questionnaire, short form (CTQ-SF). This consistsof 5 subscales: physical abuse, sexual abuse, emotional abuse, emotional neglect, and physical neglect. Assessment of depression was basedon the Calgary Depression Scale for Schizophrenia (CDSS).
Results: We found significant associations between EASE total score and CTQ total score and between EASE total score and emotionalneglect subscore in women, but not men. We also found significant associations between CDSS total score and CTQ total score and betweenCDSS total score and emotional abuse, emotional neglect, and physical neglect subscores in women, but not men. In men we did not find anysignificant associations between EASE total score, CDSS total score and any CTQ scores.
Conclusion: CT was significantly associated with higher levels of ASEs in women in the early treated phases of schizophrenia, but not inmen. This again associated with an increase in depressive symptoms.
2014 Elsevier Inc. All rights reserved.
CT also has a more long-lasting effect on the HPA axis, withsubsequent stress-sensitivity, compared to trauma in adulthood
Studies show that childhood trauma (CT) is associated with
or recent stressful events . In addition to changes in the
a wide range of psychiatric disorders and has also been
stress- and immune systems, CT has also been found to be
related to subclinical psychopathology in otherwise healthy
associated with sensitization of the mesolimbic dopamine
adults CT has a profound impact on development; an
system and concomitant changes in brain structures such as the
impact that goes far beyond the increased risks for post-
hippocampus and the amygdala , with clear indications
traumatic stress-disorders and related symptomatologies.
of gene × environment interactions
Studies also demonstrate that CT often is followed by identity
CT has repeatedly been postulated as a risk factor for
problems, affect dysregulation, and relational disturbances
developing psychotic disorders including schizophrenia, with a recent meta-analysis which includedprospective case-control studies showing a modest butstatistically significant odds-ratio . Another meta-
⁎ Corresponding author at: Innlandet Hospital Trust, Division of Mental
analysis which included retrospective studies also found a
Health, Department for Psychosis and Rehabilitation, 2840 Reinsvoll,
greater prevalence of CT among patients with a psychotic
Norway. Tel.: +47 95781487; fax: +47 61147785.
E-mail address: (E. Haug).
disorder than in the general population Trauma and
0010-440X/ 2014 Elsevier Inc. All rights reserved.
E. Haug et al. / Comprehensive Psychiatry 56 (2015) 35–41
bullying are also found to be more prevalent in persons with
biological disturbances , vulnerabilities and risk
psychotic experiences than in healthy controls and are
factors . CT appears to have a pervasive effect on
related to increased levels of depression and anxiety and a
psychopathology, but as far as we know there is no research
poorer sense of self in this group, in addition to more
investigating the relationships between CT and ASEs in
perceptual disturbances The presence of CT has also
schizophrenia. This relationship is however of interest since
been associated with specific clinical characteristics after
CT, particularly in the form of emotional maltreatment, has
onset of psychosis, including increased cognitive impair-
been linked to the phenomenon of depersonalization in the
ments, social dysfunction and dissociative symptoms
otherwise healthy persons , while severe depersonaliza-
Most studies indicate that CT is more frequently
tion can involve many experiences that resemble ASEs
present in women than in men, with suggestions that the
The main purpose of the current study was to explore the
impact of CT on later psychopathology is stronger in women
possible relationships between CT and ASEs in the early
and with one study finding the association between CT
treated phases of schizophrenia. Our main hypothesis was
and psychosis to only be present in women .
that CT is related to high levels of ASEs in schizophrenia.
Profoundly altered basic self-experience in the form of
characteristic non-psychotic disturbances of the basic senseof self is recognized as a core feature of schizophrenia .
Anomalous self-experiences (ASEs; i.e. disturbances of
2. Material and methods
basic self-awareness or sense of self) aggregate in schizo-
2.1. Design and sample
phrenia spectrum disorders , are present also in theprodromal stages and might be predictive of
The current study is part of the Norwegian Thematically
conversion to psychosis in individuals at ultra high risk
Organized Psychosis (TOP) Study . The study involved
The phenomenological concept of the self refers to
all treatment facilities in two neighboring Norwegian
here-and-now experiences associated with implicit aware-
counties (Hedmark and Oppland) with a county-wide
ness, and in this context differs from self-concepts based on
population of 375,000 people. Inclusion criteria were age
developmental theories including psychoanalytic—or self-
between 18 to 65 years, and being consecutive in- or
psychological notions of the self. The phenomenological
outpatient referred to first adequate treatment for a DSM-IV
concept of the self has three hierarchical but interconnected
diagnosis of schizophrenia spectrum psychosis (schizophre-
levels: the narrative self, the reflective self and the pre-
nia, schizophreniform disorder and schizoaffective disorder)
reflective self . The narrative self refers to explicit
in 2008 and 2009. Exclusion criteria were the presence of
experiences and recollections of the person as having
brain injury, neurodegenerative disorder, or intellectual
specific characteristics such as personality, habits, style,
disability. Patients with concurrent substance use disorders
and a personal history. The reflective self is a relatively
were included, but had to demonstrate at least 1 month
explicit, cognitive awareness of the self as an invariant and
without substance use, or clear signs that the psychotic
persisting subject of experience and action; the presence of a
disorder had started before the onset of significant substance
relatively stable "I" over time. The pre-reflective self is the
use (i.e. did not meet the criteria for substance induced
most basic level of self-awareness and refers to the first-
person quality of a person's experiences, i.e. the tacit
A total of 55 patients early in their treatment course
awareness that this is "my" experience. This level of
completed the full protocol including the Examination of
selfhood is fully implicit in—and inseparable from—the
Anomalous Self-Experience (EASE) interview measur-
experience itself. ASEs are subjective experiences that
ing ASEs. Coming to first adequate treatment was defined as
include certain and subtle forms of depersonalization,
not having previously received adequate antipsychotic
anomalous experiences of cognition and stream of con-
medication (adequate doses for 12 weeks, or until
sciousness, self-alienation, pervasive difficulties in grasping
remission), or any treatment at all. Some of the patients
familiar and taken-for-granted meanings, unusual bodily
had not even initiated their first treatment at the time of
feelings, permeability or complete loss of the self-world
inclusion. To enhance statistical power, we also included 11
boundary, in addition to existential reorientation These
patients consecutively enrolled in a closely related ongoing
are fundamental distortions of the first-person perspective,
study of young psychosis patients born in 1985/86. They met
including deficiencies in the sense of being a coherent
the same inclusion and exclusion criteria except for the strict
subject or a self-coinciding center of action, thought and
definition of first treatment. They were, however, in an early
experience Phenomenology is focused on experiential
phase of their treatment course, with an even shorter
phenomena and not on the search for underlying mecha-
duration of untreated psychosis (DUP) than the strict first
nisms or etiology. ASEs are from this perspective core
treatment patients.
features of schizophrenia, and thus carry the same complex
All participants gave written, informed consent to
etiology as the disease itself. Recent research has however
participate. The study was approved by the Regional
addressed the pathogenic role of ASEs in schizophrenia ,
Committee for Medical Research Ethics and the Norwegian
and the relationship between ASEs and underlying neuro-
Data Inspectorate.
E. Haug et al. / Comprehensive Psychiatry 56 (2015) 35–41
2.2. Clinical assessments
the level of lifetime occurrence of ASEs. Each EASEinterview lasted 30–90 minutes. EH was trained by one of
Diagnoses were ascertained by two experienced psychia-
the authors of the EASE (PM), and conducted all the
trists using the Structural Clinical Interview for the Diagnostic
interviews. The inter-rater reliability (IRR) for the EASE
and Statistical Manual of Mental Disorders, fourth edition
items was found to be very good .
(SCID-IV) . Symptom severity and function were assessedusing standard psychiatric measures including the Structured
2.5. Statistical analysis
Clinical Interview for the Positive and Negative SyndromeScale (SCI-PANSS) Duration of untreated psychosis
All analyses were performed with the statistical package
(DUP) was measured as time from onset of psychosis (first
SPSS, version 18.0. Mean and standard deviations are
week with a score of four or more on one of the of the PANSS
reported for continuous variables and percentages for
subscale items: delusions, hallucinatory behavior, grandiosity,
categorical variables. We examined bivariate associations
suspiciousness/persecution or unusual thought content).
(nonparametric correlations) between the 5 subscales of
Assessment of depression was based on the Calgary
CTQ and EASE total score in addition to symptoms as
Depression Scale for Schizophrenia (CDSS) . Both raters
measured by PANSS subscales and CDSS. A two-way
completed the TOP study group's training and reliability
analysis of variance was conducted to explore the impact of
program with SCID training based on and supervised by the
CT and gender on levels of ASEs. In the analyses of CTQ
UCLA training program For DSM-IV diagnostics, mean
subscales, we controlled for multiple comparisons using
overall kappa for the standard diagnosis of training videos for
Bonferroni adjustments i.e. with a p-value of 0.01 as the
the study as a whole was 0.77, and mean overall kappa for a
level of statistical significance. Multiple regression analysis
randomly drawn subset of study patients was also 0.77 (95%
was used to control for CDSS total score as a covariate.
CI 0.60–0.94). Intra class coefficients (ICC 1.1) for the otherscales were: PANSS positive subscale 0.82 (95% CI 0.66–
0.94), PANSS negative subscale 0.76 (95% CI 0.58–0.93),PANSS general subscale 0.73 (95% CI 0.54–0.90), and GAF-F
presents the sociodemographic and clinical
0.85 (95% CI 0.76–0.92).
features of the sample, including the mean scores of theCTQ. The mean EASE total score is in accordance with other
2.3. Assessment of childhood trauma
studies on ASEs, and significantly higher than in other
Data on CT were collected using the Norwegian version
mental disorders . There were no significant gender
of the Childhood Trauma Questionnaire, short form (CTQ-
differences in the number of patients reporting childhood
SF) . This is a 28-item self-report inventory, developed
trauma. This was also the case for physical abuse, sexual
and validated based on the original 70-item version , that
abuse, emotional abuse, emotional neglect, and physical
provides a relatively short screening of maltreatment
neglect subscale scores ).
experiences before the age of 18. It comprises 28 items,
For the whole sample taken together we did not find any
yielding scores on 5 subscales of trauma: physical abuse,
significant associations between EASE total score and CTQ
sexual abuse, emotional abuse, emotional neglect, and
total score, or between EASE total score and CTQ subscores.
physical neglect. For estimates of frequencies of childhood
We found a significant association between current depres-
trauma we used the moderate to severe predefined cutoff
sion (CDSS total score) and CTQ total score. In addition, we
suggested by Bernstein of ≥10 for physical abuse, ≥8
found significant associations between CDSS score and
for sexual abuse, ≥13 for emotional abuse, ≥15 for
EASE total score (not in table; r = .319, p = .018) and
emotional neglect, and ≥10 for physical neglect.
2.4. Assessment of anomalous self-experiences
Demographic and clinical characteristics.
Number of patients
ASEs were assessed using the EASE manual
comprising five domains: (1) Cognition and stream of
Male gender, n (%)
consciousness. (2) Self-awareness and presence. (3) Bodily
Age years, mean (SD)
experiences. (4) Demarcation/transitivism. (5) Existential
DUP weeks, median (range)
reorientation. This represents a wide variety of anomalous
self-experiences condensed into 57 main items and scored on
a 5-point Likert scale (0–4), in which 0 = absent; 1 =
questionably present; 2 = definitely present, mild; 3 =
definitely present, moderate; 4 = definitely present, severe.
For the purpose of the analyses, the resulting scores were
dichotomized into 0 (absent or questionably present) and 1
Emotional neglect
(definitely present, all severity levels). The EASE measures
E. Haug et al. / Comprehensive Psychiatry 56 (2015) 35–41
lower levels of current depression in men compared to
Childhood trauma report (CTQ subscales).
women. Mean CDSS score was 7.1 (SD 4.0) in men and 11.1
(SD 7.0) in women (p = 0.033) (not in table). In men we did
not find any significant associations between EASE total
score and CTQ based scores, nor between CDSS total score
and any CTQ scores
4.1. General discussion
Our main finding was that childhood trauma (CTQ total
score) was significantly associated with high levels of
anomalous self-experiences (ASEs/EASE total score) in the
early treated phases of schizophrenia in women, but not in
men. This seemed to be specifically driven by the level of
a Mann Whitney U test.
emotional neglect; as shown by significant associations
b Moderate to severe cutoff scores: ≥10 for physical abuse, ≥8 for
between ASEs and this subscale, but not other subtypes of
sexual abuse, ≥13 for emotional abuse, ≥15 for emotional neglect, and ≥10
childhood trauma. The level of ASEs as indicated by the
for physical neglect).
EASE total score was the same as in previous studies of
Fisher's exact test.
schizophrenia populations ; comparable to levelsreported in ultra high risk populations and significantlyhigher than in healthy controls or non-schizophrenia
between CDSS score and sexual abuse, emotional abuse,
spectrum disorders .
emotional neglect subscores ). A two-way analysis
Our findings are consistent with previous studies that
of variance indicated a trend-level effect of emotional
show a stronger association between CT and clinical
neglect on EASE total score (p = 0.04), with an additional
manifestations of psychiatric disorders in women
significant interaction effect between gender and emotional
Although most studies indicate that women report a higher
neglect on EASE total score ().
prevalence of childhood trauma than men, there were no
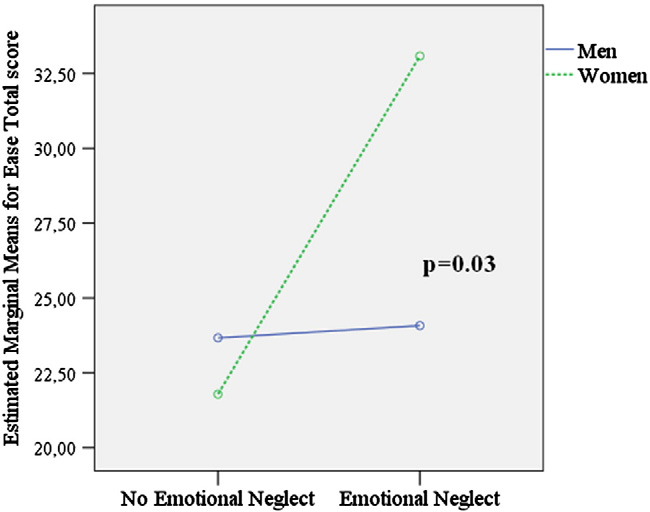
In follow-up analyses investigating genders separately,
such gender differences in the current study. The lack of
we found highly statistically significant associations between
associations between ASEs and emotional neglect in men
EASE total score and CTQ total score and between EASE
could thus not simply be due to less statistical power in the
total score and emotional neglect subscore in women
(). We also found statistically significant associations
We also found a statistically significant association
between CDSS total score and CTQ total score and between
between CT and current depression in women, in line with
CDSS total score and emotional abuse, emotional neglect,
several studies demonstrating a firm link between CT and the
and physical neglect subscores in women (). When
risk of depression and with studies suggesting that
CDSS total score was introduced as a covariate, the
emotional maltreatments may have particular effects on the
significant association between EASE total score and CTQ
development of negative self-image and depression In
scores was no longer apparent. There were significantly
particular, emotional neglect in childhood has been
Table 3Correlation (Spearman's rho) between childhood trauma (CTQ scores) and anomalous self-experiences, and between childhood trauma and depression.
Emotional neglect
(EASE total score)
Depression (CDSS total score)
⁎ Correlation is significant at the 0.01 level (2-tailed).
E. Haug et al. / Comprehensive Psychiatry 56 (2015) 35–41
4.2. Strengths and limitations of the study
We included patients in the early phase of the treated course
of the disorder, thereby minimizing potential confoundingeffects such as selection of non-responders and chronicity thatmight impact on the assessment of ASEs and CT. TheNorwegian mental health care offers public mental health careto all individuals with mental illness within a given catchmentarea. Because of the absence of private mental health care inNorway, the sample is not biased for socioeconomic class. Thestudy population is representative because we included allconsecutive in- or outpatients referred to treatment for apsychotic disorder in two neighboring Norwegian counties in adefined time period.
4.2.2. Limitations
Fig. 1. Interaction between gender and emotional neglect on EASE total
The correlational nature of this study gives no firm
score.ANOVA, interaction between gender and emotional neglect: Df = 1,f = 4.91, p = 0.03.
conclusions about the direction of associations, or about
"No emotional neglect," n = 29; "emotional neglect,"
n = 25; men, n = 28; women, n = 26.
causality. CT ratings are made from retrospective self-reports, and childhood adversities might be both conse-quences and triggers of distorted self-experiences. Highlevels of ASEs and high levels of CT reported could also be a
associated with hippocampal and striatal alterations in adults
result of recall bias among patients with high levels of
. Sex differences in stress-reactivity, including in the
depression. However, the retrospective examination of CT in
development of the stress-sensitive cortico-striatal-limbic
patients with psychosis has been found to be a valid and
regions could partly explain why CT contributes
reliable source when collecting data in previous studies .
differently to risk for depression in women and men in linewith previous indications that women might be more
susceptible to the negative effects of stress and toearly trauma in general. The presence of ASEs is today
Childhood trauma was significantly associated with
most often viewed as a stage in the development of
higher levels of ASEs (EASE total score) in women in the
schizophrenia . The results of this study could
early treated phases of schizophrenia. This seemed to be
indicate that CT adds to this particular development.
specifically driven by emotional abuse, emotional neglect
There are several possible explanations of the link between
and physical neglect. Our data support including emotional
CT, ASEs and depression. It is well-known that CT is a risk
abuse, emotional neglect and physical neglect in addition to
factor for the development of depression. If CT also increases
the more frequently investigated sexual abuse and physical
the risk of ASEs in susceptible individuals, the link between
abuse when investigating associations between CT and pre-
ASE and depression could either be a statistical artifact or
psychotic and psychotic features.
indicate that the presence of ASEs further increases the risk ofdepression. A model where depression mediates the effect ofCT on ASEs in the strict definition of the term is, however,
Role of funding source
unlikely, since ASEs and CT are thought to be relatively stableover time, while depression fluctuates. We can however not
Funding for this study was provided by Innlandet
completely rule out that depressive individuals could be biased
Hospital Trust (grant number 150229). The funding source
towards reporting both more CTs and more ASEs. Empirical
had no further role in study design; in the collection, analysis
studies documenting the stability of ASEs over time are thus
and interpretation of data; in the writing of the report; and in
required. Finally, as we know that ASEs are present before the
the decision to submit the paper for publication.
onset of psychosis and thus could potentially be presentalready in childhood and adolescence , they could interactwith difficulties in eliciting or receiving emotional support,
which in turn could increase the risk of depression. Analternative explanation could be that females have a more
EH, IM, PM, MØ and BN planned the current study, and
complex response to trauma involving more ASE-like
OAA contributed to the study design. EH and UB
depersonalization and dissociation like phenomena
contributed to data collection. EH conducted the statistical
. However, the lack of gender differences in relevant
analyses and also wrote the first draft of the manuscript. EH,
EASE subscales does not support this hypothesis at present.
IM and MA contributed to the analyses. All authors
E. Haug et al. / Comprehensive Psychiatry 56 (2015) 35–41
participated in critical revision of manuscript drafts and
approved the final version.
Author disclosure
All authors declare no conflict of interest.
The authors thank the patients for participating in the
study. We also thank Innlandet Hospital Trust for making
convenient and necessary arrangements for the work on this
article. BN was supported by an NHMRC Career Develop-
ment Fellowship (#1027532).
E. Haug et al. / Comprehensive Psychiatry 56 (2015) 35–41
Source: http://easenet.dk/wp-content/uploads/2016/03/Haug-2015-Anomalous-self-experience-and-childhood-trauma-in-first-episode-schizophrenia.pdf
Tadalafil (Adcirca®) Issued by PHA's Scientific Leadership Council Information is based on the United States Food and Drug Administration drug labeling Last Updated November 2013 WHAT IS TADALAFIL? Tadalafil is an oral medication called a phosphodiesterase-5 (PDE5) inhibitor approved for the treatment of pulmonary arterial hypertension (PAH) in World Health Organization (WHO) Group 1
Symptom control in the last days of life Owner Anne Garry Contributions from Specialist Palliative Care teams in York and Scarborough Jane Crewe, Lynn Ridley and Diabetes team Version 3 Date of issue December 2014 Review date December 2017 Principles of symptom management in last days of life These principles are applicable to the care of patients who may be dying from any cause Recognise that death is approaching Studies have found that dying patients will manifest some or all of the following: