Levitra enthält Vardenafil, das eine kürzere Wirkdauer als Tadalafil hat, dafür aber schnell einsetzt. Männer, die diskret bestellen möchten, suchen häufig nach levitra kaufen ohne rezept. Dabei spielt die rechtliche Lage in der Schweiz eine wichtige Rolle.
Ley-lab.liai.org
Rosiglitazone Reduces the Accelerated Neointima Formation
After Arterial Injury in a Mouse Injury Model of
Type 2 Diabetes
J. William Phillips, MD; Kurt G. Barringhaus, MD; John M. Sanders, BS; Zandong Yang, MD;
Meng Chen, MD; Sean Hesselbacher, BS; Ann C. Czarnik, BS; Klaus Ley, MD;
Jerry Nadler, MD; Ian J. Sarembock, MB, ChB, MD
Background—Hyperglycemia (HG) and hyperinsulinemia (HI) may be factors enhancing the atherosclerotic complications
of diabetes. We hypothesized that specific feeding of C57BL/6 apolipoprotein (apo) E⫺/⫺ mice would alter theirmetabolic profiles and result in different degrees of neointima (NI) formation. We additionally hypothesized that aninsulin-sensitizing agent (rosiglitazone) would prevent the development of type 2 diabetes and reduce neointimaformation after carotid wire injury measured at 28 days.
Methods and Results—Fasting glucose and insulin levels were elevated in the Western diet (WD) group, with a trend
toward higher insulin levels and euglycemia in the fructose diet (FD)–fed mice. NI formation was exaggerated in theWD group compared with the FD or chow control groups. In the WD mice given rosiglitazone, glucose and insulinlevels remained normal and NI formation was significantly reduced, as was NI macrophage content.
Conclusions—These findings demonstrate that apoE⫺/⫺ mice fed a WD develop type 2 diabetes with an exaggerated NI
response to injury. FD mice maintain euglycemia but develop insulin resistance, with an intermediate degree of NI
growth compared with chow diet controls. Rosiglitazone prevents the development of hyperglycemia and hyperinsu-
linemia and normalizes the insulin release profile in the apoE⫺/⫺, WD-fed mouse and significantly reduces NI formation
by 65% after carotid wire injury while reducing macrophage infiltration. These data support the hypothesis that type 2
diabetes in the setting of elevated cholesterol accelerates the response to vascular injury and suggest that agents that
improve insulin sensitivity may have therapeutic value in reducing restenosis in type 2 diabetes.
(Circulation. 2003;108:
1994-1999.)
Key Words: angioplasty 䡲 drugs 䡲 hypercholesterolemia 䡲 diet 䡲 diabetes mellitus
Atherosclerotic vascular disease is a major cause of These mice do not develop significant hypercholesterolemia,
increased morbidity and mortality in humans with type
and the spontaneous lesions that develop are immature and
2 diabetes mellitus.1,2 The present trend of increased obesity
have a restricted anatomic distribution.5,7 The generation of
is predicted to significantly increase the incidence of type 2
the apolipoprotein E– deficient (apoE⫺/⫺) mouse on the
diabetes in the United States population.3 Although the
C57BL/6 background has provided a model that develops
prevalence of atherosclerosis is increased in type 2 diabetes,
severe hypercholesterolemia and atherosclerosis throughout
the underlying mechanisms responsible remain poorly under-
the arterial tree that is accelerated on a WD.8–10 In addition,
stood.4 The in vivo study of the interactions and contributions
a high-fructose diet (FD) has been reported to induce hyper-
of hyperglycemia, hyperinsulinemia, and hypercholesterol-
insulinemia, with insulin resistance and euglycemia in
emia in the development of atherosclerosis and the response
rats.11,12 Rats, however, generally do not develop hypercho-
to vascular injury in type 2 diabetes has been limited by
lesterolemia and do not develop significant atherosclero-
available animal models that develop all of these metabolic
sis.13,14 The normal pattern of insulin secretion has been
shown to be biphasic both in isolated perfused preparations of
The C57BL/6 mouse strain has been shown to develop
rat pancreatic islets in vitro and in humans.15–17
diet-induced type 2 diabetes and atherosclerosis when fed a
Peroxisome proliferator–activated receptor-␥ has been
high-fat, Western diet (WD) for prolonged periods of time.5,6
shown to be expressed in many of the cells that play a role in
Received September 24, 2002; de novo received March 20, 2003; revision received June 16, 2003; accepted June 17, 2003.
From the Departments of Medicine (J.W.P., K.G.B., J.M.S., S.H., A.C.C., J.N., I.J.S.), Cardiovascular Division, and Cardiovascular Research Center
(K.L., I.J.S.), Division of Endocrinology (Z.Y., M.C., J.N.), and Department of Biomedical Engineering (K.L.), University of Virginia Health System,Charlottesville, Va.
This work was supported by an unrestricted grant from GlaxoSmith-Kline.
Correspondence to Ian J. Sarembock, MD, Cardiovascular Division, University of Virginia Health System, Box 800158, Charlottesville, VA
22908-0158. E-mail
[email protected]
2003 American Heart Association, Inc.
Circulation is available at http://www.circulationaha.org
Phillips et al
Type 2 Diabetes Mellitus in apoEⴚ
/ⴚ
Mice
the response to vascular injury and modulates the actions that
are thought to initiate neointimal (NI) growth, including
Sections were stained for macrophage/foam cells using an anti-
inflammation.18–24 Three different thiazolidinediones, rosigli-
mouse macrophage mAb F4/80 (Accurate Chemical and Scientific
tazone, pioglitazone, and troglitazone, have been shown to
Corp) or for smooth muscle actin–positive cells using mAb 1A4(Dako Corp). For quantitative immunocytochemical comparisons of
prevent spontaneous atherosclerosis in the aorta of LDLR⫺/⫺
macrophage content or smooth muscle cell content, sections were
mice or in balloon-injured rat carotid arteries but have not
digitized and the number of positively stained pixels were counted
been studied in a model of arterial injury in the setting of
and normalized to total NI and medial area using Image Pro Plus 3.0
hypercholesterolemia.25–27 This is important, because these
agents, which are ligands for peroxisome proliferator–acti-vated receptor-␥, are used in the treatment of patients with
type 2 diabetes who often have concomitant hypercholester-
Blood glucose levels were assessed before initiation of diets, after 1week of diet, and at the time of euthanasia by glucometer (Accu-
check Advantage; Roche). In addition, fasting glucose, insulin, and
lipid panels were assessed at the time of euthanasia after 5 weeks of
Based on these data, we hypothesized that C57BL/6
the respective diets. Blood samples at the time of euthanasia were
apoE⫺/⫺ mice fed a WD would develop hypercholesterolemia
drawn by cardiac puncture into serum separator tubes (Becton-
with a metabolic profile of hyperinsulinemia and hypergly-
Dickinson). Lipid levels were determined by the University ofVirginia Clinical Pathology Laboratory.
cemia with an insulin release profile consistent with type 2diabetes whereas apoE⫺/⫺ mice fed a FD would develop
Pancreatic Islet Isolation
hypercholesterolemia with hyperinsulinemia but euglycemia
At the time of euthanasia, before perfusion fixation, the pancreas of
and an insulin release profile consistent with the metabolic
each mouse was removed and prepared for histology or islet cells
syndrome. We additionally hypothesized that in the setting of
isolated for glucose perifusion and insulin release kinetics. Mouse
carotid wire injury, NI growth would be accelerated in the
pancreatic islets were isolated using a method modified from
WD mice and that treatment with an insulin-sensitizing agent
previously published protocols.32,33 Briefly, after exposition of thepancreas, the common duct of bile was cannulated and injected with
(rosiglitazone) would prevent the development of type 2
Hanks' solution containing 0.7 to 1 mg/mL Collagenase P (Roche
diabetes and reduce NI formation after carotid wire injury at
Molecular Biochemicals) and the dissected pancreas was digested at
28 days in the apoE⫺/⫺, WD-fed mouse.
37°C. Pancreatic islets were separated from pancreatic digest byFicoll density gradients (Sigma). Islets were individually picked,washed, and cultured overnight at 37°C in 5% CO in M199 medium
(Life Technologies) supplemented with 10% FCS and antibiotics.
Animals
Female C57/BL6 apoE⫺/⫺ mice 8 to 10 weeks of age (18 to 20 g; The
Measurement of Insulin Release in a
Jackson Laboratory, Bar Harbor, Me) were used for these experi-
ments. Animals were handled in compliance with the
Guiding
The isolated pancreatic islets of Langerhans from the mice were
Principles in the Care and Use of Animals. Protocol approval was
subjected to overnight culture in RPMI1640 medium (GIBCO)
obtained from the Animal Research Committee of the University of
supplemented with 10% FBS in a tissue culture incubator (37°C, 5%
Virginia Health System.
CO ). After overnight culture, 100 islets from each diet-fed group of
mice were transferred to a perifusion chamber. The temperature was
Mouse Injury Model
maintained at constant 37°C. The islets were perifused at a rate of 1
The mouse carotid artery wire injury model of Lindner et al28 was
mL/min using a multichannel peristaltic pump (Harvard Instruments)
used with minor modification, as we have previously published.29,30
with Krebs-Ringer bicarbonate (KRB) buffer (pH 7.4), continuously
Mice (N⫽10 per group) were fed either a WD (TD 88137, Harlan-
gassed with 95% oxygen and 5% carbon dioxide, and supplemented
Teklad; containing 21% fat by weight, 0.15% by weight cholesterol,
with 20 mmol/L HEPES, 0.1% BSA, and glucose as required. The
and 19.5% by weight casein without sodium cholate), a FD (TD
preliminary perifusion was performed for 30 minutes with KRB
96130, Harlan-Teklad; containing 13% of calories from fat, 67%
containing 3.0 mmol/L glucose to obtain stable baseline insulin
from carbohydrates, 20% from protein), a chow diet (CD), or a WD
secretion. The perifusion medium was then rapidly replaced by KRB
with rosiglitazone (10 mg/kg per day, GlaxoSmithKline) for 1 week
containing 30 mmol/L glucose and sustained for 60 minutes. The
before and 4 weeks after carotid injury.
perifusion medium was switched back to KRB containing3.0 mmol/L glucose for another 30 minutes. The perifusate from
each chamber was collected at 1-minute intervals, and 25 L ofperifusate from each collected sample was analyzed for insulin
The arterial segments were dehydrated in ethanol and xylene and
concentration (microgram per milliliter) using EIA (ALPCO) with
embedded in paraffin. Sections (5 m thick) were stained by the
crystalline mouse insulin as standard. The insulin secretion profiles
Movat method.31 Histomorphometric analysis was performed by
from islets of each of the 3 diet-fed groups were generated by
individuals blinded to type of diet. For quantitative histopathologic
plotting the perifusate insulin contents against the duration of
comparisons, the mean of 10 sections was taken. The area of the
lumen, internal elastic lamina (IEL), and external elastic lamina(EEL) were determined by planimetry using Image Pro Plus 3.0(Media Cybernetics), and the lumen area, plaque area, medial area,
intima to media ratio, and overall vessel area were calculated. NI
Statistical analysis was performed using NCSS 97. Data are reported
area was calculated by subtracting lumen area from the IEL area, and
as the number of carotid arteries in each group, and plaque area and
medial area was determined by subtracting the IEL area from the
intima to media ratio are expressed as mean⫾SD. Data were
EEL area. Arterial size was measured by tracing the circumference
compared using ANOVA and Student's
t test to evaluate 2-tailed
levels of significance.
October 21, 2003
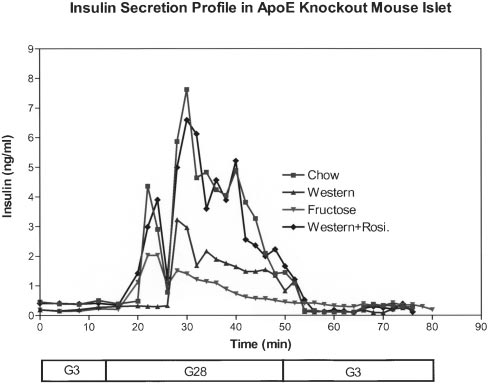
Figure 2. Pancreatic islet insulin release kinetics. Insulin release
profiles from pancreatic islet cells after perifusion of glucose
demonstrating loss of the first peak and an attenuated second
peak in WD animals, consistent with a pattern of type 2 diabe-
tes with normalization of this pattern in the WD animals treated
with rosiglitazone. Note the attenuation of both first and second
peaks in FD animals, consistent with insulin resistance and a
normal biphasic release profile in CD animals (n⫽10 animals per
group with 100 islets isolated per diet-fed group for perifusate
insulin levels).
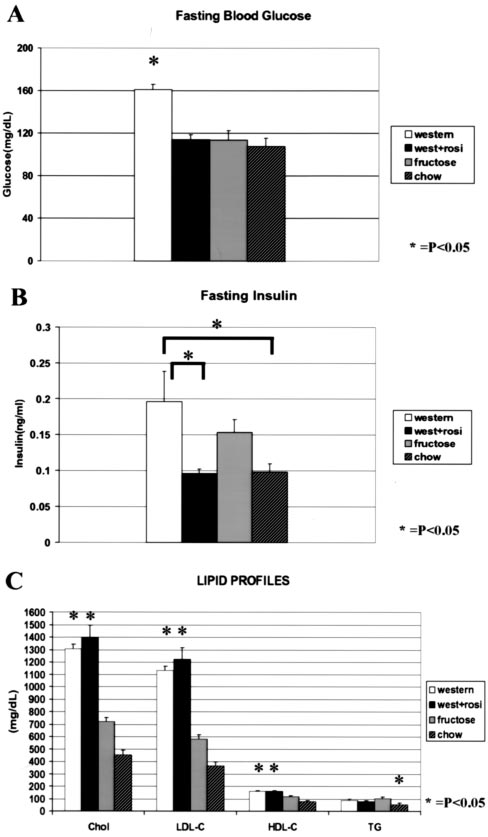
nonsignificant trend toward higher insulin levels in the FDgroup at 5 weeks (Figure 1B). Insulin levels in the WD groupwith rosiglitazone remained normal (Figure 1B). Insulinrelease profiles from pancreatic islet cells with perifusion ofglucose demonstrated loss of the first-release peak and anattenuated second-release peak in WD animals, consistentwith a pattern of type 2 diabetes. In contrast, rosiglitazone-treated, WD-fed mice had normal release kinetics, similar tothe CD animals, which demonstrated a normal biphasicrelease profile. Attenuation of both first and second peaks
Figure 1. Metabolic profiles. A, Fasting blood glucose in the WD
was observed in FD animals, consistent with a pattern of
mice vs FD or CD after 5 weeks of diet. Note the significantly
insulin resistance (Figure 2).
higher fasting glucose levels in the WD group vs FD or CD(*P⬍0.05). Rosiglitazone therapy in the WD-fed mice results inmaintenance of normoglycemia. B, Fasting insulin levels were
significantly higher in the WD vs CD group, with a nonsignificant
A graded elevation in total cholesterol, LDL, and HDL levels
trend toward higher insulin levels in the FD group after 5 weeks
was observed in the WD versus FD and CD groups. Triglyc-
on feed. Rosiglitazone therapy in the WD mice results in insulinlevels similar to those of the CD group. C, Total cholesterol,
eride levels were elevated in both the Western and FD
LDL, and HDL levels in the WD, FD, and CD groups. A graded
animals (Figure 1C). Total cholesterol, LDL, and HDL levels
elevation in total cholesterol, LDL, and HDL levels was observed
were elevated in the WD with rosiglitazone group to a level
in the WD vs FD and CD groups. Triglyceride levels were ele-vated in the WD and FD animals, and WD mice with rosiglita-
that was equal to that seen in the WD-alone group (Figure
zone had levels that were no different than the WD-only group.
Histomorphometry
There were no differences in the extent of injury between any
Metabolic Profiles and Insulin Release Kinetics
of the groups as defined by number of elastic laminae broken
Baseline glucose levels were normal in all groups before
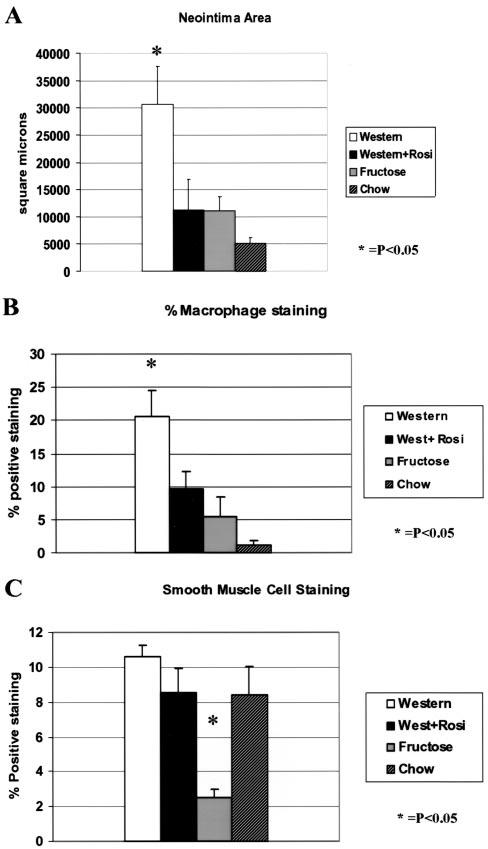
(data not shown). At 28 days after carotid wire injury, NI
initiation of diets and after 1 week of feeding at the time of
formation was significantly greater in the WD group com-
carotid wire injury (data not shown). After 5 weeks on diet, at
pared with the FD group (31 000⫾7000 m2 versus
the time of euthanasia (Figure 1A), fasting glucose levels
11 000⫾2500 m2, Pⱕ0.05, n⫽10 per group). The FD group
were higher in the WD group versus FD or CD groups
had significantly greater NI than the CD group (11 000⫾2500
whereas glucose levels in mice fed a WD plus rosiglitazone
m2 versus 5130⫾1000 m2, Pⱕ0.05, n⫽10 per group)
remained normal. Fasting insulin levels were significantly
(Figure 3A). There was a significant 65% reduction in NI
higher in the WD group compared with CD group, with a
formation in the WD group treated with rosiglitazone com-
Phillips et al
Type 2 Diabetes Mellitus in apoEⴚ/ⴚ Mice
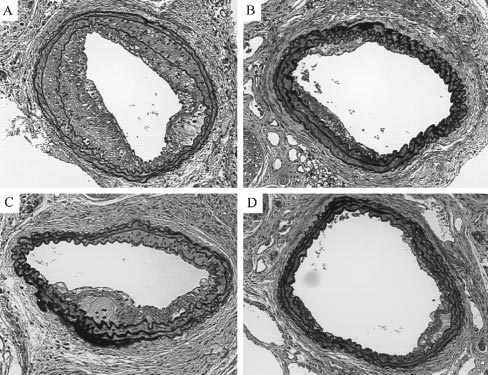
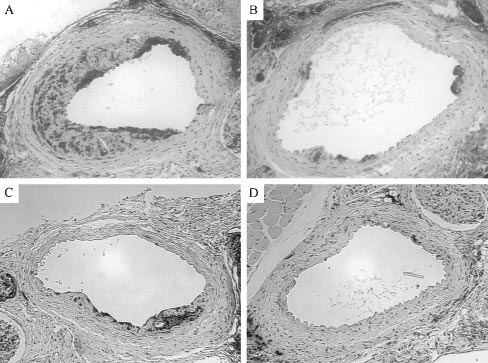
Figure 4. Representative examples of Movat-stained injured left
carotid arteries (LCA) from a mouse fed a WD showing robust
NI formation (A), a mouse fed a WD with rosiglitazone treatment
illustrating significantly less NI growth (B), a mouse fed a FD
with moderate NI growth (C), and a mouse fed CD showing min-
imal NI growth (D). Magnification ⫻200.
the other groups (Figure 3C). Representative examples ofMOVAT-stained arteries from each group are shown inFigures 4A through 4D, immunostaining for macrophages isshown in Figures 5A through 5D, and smooth muscle cellsare shown in Figures 6A through 6D. There was no signifi-cant difference in either media or EEL areas between groups(data not shown).
This is the first study to document a range of metabolicprofiles consistent with type 2 diabetes and insulin resistancein C57BL/6 apoE⫺/⫺ mice fed various diets. We show gradedNI formation after arterial injury being most robust in thesetting of type 2 diabetes plus hyperlipidemia. On a CD, the
Figure 3. Histomorphometry and immunohistochemistry. A,
apoE⫺/⫺ mouse develops mild but significant hypercholester-
Quantitative histomorphometry of plaque area in injured carotidarteries 4 weeks after wire denudation and 5 weeks on a WD,FD, CD, or WD with rosiglitazone. Note the markedly increasedneointimal growth in the apoE⫺/⫺ mice fed a WD compared withthe FD or CD mice, *P⬍0.05. Also, note the significantly morerobust NI growth in the FD group vs the CD group, *P⬍0.05. B,Quantitative immunocytochemistry of macrophage infiltrationinto the wall of injured carotid arteries 4 weeks after denudationand 5 weeks on respective diets. Note the marked reduction inpercent area occupied by macrophages in the WD with rosigli-tazone group compared with the WD group, *P⬍0.05. In addi-tion, the FD and CD groups have significantly less macrophagestaining compared with the WD group. C, Smooth muscle cellstaining demonstrating significantly less staining in the FD groupcompared with the other groups, *P⬍0.05.
pared with the WD group (11 000⫾5000 m2 versus31 000⫾6000 m2, Pⱕ0.05, n⫽10 per group). Macrophagecontent in the injured vessel wall was significantly reducedby 52% in the WD group treated with rosiglitazone comparedwith WD alone (9.5⫾2% versus 20⫾4%, Pⱕ0.05, Figure3B). Fewer macrophages were seen in the FD and chow
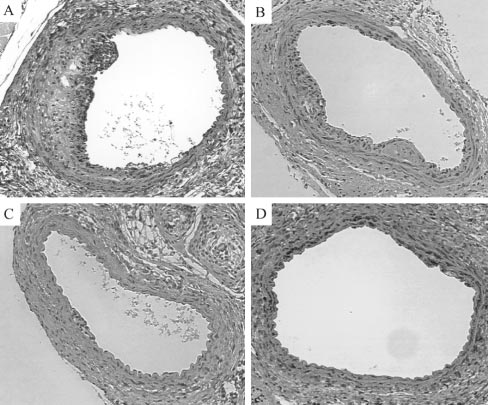
Figure 5. Macrophage content. Representative immunostaining
groups compared with the WD group (5.5⫾2% and 1⫾0.8%,
for macrophages using the F4/80 anti-mouse macrophage mAbfrom a mouse fed a WD (A), a mouse fed a WD with rosiglita-
Pⱕ0.05, Figure 3B). There was also significantly less stain-
zone (B), a mouse fed a FD (C), and a mouse fed CD (D). Mag-
ing for smooth muscle cells in the FD group compared with
nification ⫻200.
October 21, 2003
addition, compared with the development of insulin resis-tance, as determined by insulin release profiles in our apoE⫺/⫺mice fed a FD, the LDLR⫺/⫺ mice did not develop insulinresistance while on a FD.35 Previous studies in the LDLR⫺/⫺mice have shown a reduction in lesion formation in malemice treated with thiazolidinediones but not female mice, aswe report in our experiments.25,26 It is important to note thatthese studies evaluated spontaneous atherosclerosis in theaortic cusp and aorta in contrast to the model of arterial injuryand carotid lesion formation in our experiments. It hasrecently been shown that injury-induced NI hyperplasia anddiet-induced spontaneous atherosclerosis are controlled bydistinct sets of genes and responses to each can vary withinand between mouse strains.36
In summary, we demonstrate that apoE⫺/⫺ mice fed a WD
develop severe hypercholesterolemia and a metabolic profileconsistent with type 2 diabetes and have an exaggeratedresponse to arterial injury. The development of type 2
Figure 6. Smooth muscle cell content. Representative immuno-
diabetes in the WD-fed apoE⫺/⫺ mouse can be prevented by
staining for smooth muscle cells from a mouse fed WD (A), amouse fed WD with rosiglitazone (B), a mouse fed FD (C), and a
rosiglitazone treatment, and NI formation and macrophage
mouse fed CD (D). Magnification ⫻200.
content can be significantly reduced. This model thus pro-vides a valuable tool to study the interaction between athero-
olemia with elevated LDL cholesterol levels. The fasting
sclerosis, diabetes, and inflammation.
glucose and insulin levels on this diet remain in the normalrange, and the dynamic insulin release from isolated pancre-
atic islet cells in the face of varying glucose concentrations
This work was supported by an educational grant from GlaxoSmith-
also remains normal, characterized by preservation of the first
Kline, NIH/NHLBI Training Grant T32 HL-07355 (Dr Phillips, PI),
and second insulin release peaks. The response to arterial
Grant PO1-55798 (to Dr Nadler), NIH Grant DK-55240 (to DrChen), and the Iacocca Foundation (to Dr Yang).
injury at 28 days is minimal.
The intermediate injury response observed in the FD-fed
apoE⫺/⫺ mice that develop insulin resistance is concordant
1. Garcia MJ, McNamara PM, Gordon T, et al. Morbidity and mortality in
with a recent report in humans where in-stent restenosis was
diabetics in the Framingham population: sixteen year follow-up study.
significantly more common in patients with the metabolic
syndrome undergoing percutaneous coronary interventions.34
2. Kannel WB, McGee DL. Diabetes and cardiovascular disease: the Fra-
mingham study. JAMA. 1979;241:2035–2038.
Arterial injury in the FD group results in a 2-fold increase in
3. Mokdad AH, Serdula MK, Dietz WH, et al. The spread of the obesity
NI growth compared with the CD group. In contrast, the WD
epidemic in the United States, 1991–1998. JAMA. 1999;282:1519 –1522.
mice develop more severe hypercholesterolemia, markedly
4. Pyorala K, Laakso M, Uusitupa M. Diabetes and atherosclerosis: an
elevated LDL cholesterol levels, and modest increases in
epidemiologic view. Diabetes Metab Rev. 1987;3:463–524.
5. Paigen B, Ishida BY, Verstuyft J, et al. Atherosclerosis susceptibility
triglycerides, as has been previously reported, while devel-
differences among progenitors of recombinant inbred strains of mice.
oping the most exaggerated injury response.9,10
Arteriosclerosis. 1990;10:316 –323.
In the setting of arterial injury, the apoE⫺/⫺ mouse on a WD
6. Surwit RS, Kuhn CM, Cochrane C, et al. Diet-induced type II diabetes in
develops robust NI formation. This may be in part attributable
C57BL/6J mice. Diabetes. 1988;37:1163–1167.
7. Schreyer SA, Wilson DL, LeBoeuf RC. C57BL/6 mice fed high fat diets
to the hyperglycemia, hyperinsulinemia, and increased in-
as models for diabetes-accelerated atherosclerosis. Atherosclerosis. 1998;
flammatory response to injury compared with the FD and CD
mice. This is supported by the significant 65% reduction in
8. Nakashima Y, Plump AS, Raines EW, et al. ApoE-deficient mice develop
lesions of all phases of atherosclerosis throughout the arterial tree. Arte-
NI formation seen in WD mice treated with rosiglitazone and
rioscler Thromb. 1994;14:133–140.
a 53% reduction in macrophage content. Rosiglitazone ther-
9. Piedrahita JA, Zhang SH, Hagaman JR, et al. Generation of mice carrying
apy of WD-fed mice reduced NI formation and macrophage
a mutant apolipoprotein E gene inactivated by gene targeting in
content that approached that of the FD group but not that of
embryonic stem cells. Proc Natl Acad Sci U S A. 1992;89:4471– 4475.
10. Plump AS, Smith JD, Hayek T, et al. Severe hypercholesterolemia and
the CD mice. This could be the result of the markedly
atherosclerosis in apolipoprotein E-deficient mice created by homologous
elevated lipid levels that were not reduced by treating with
recombination in ES cells. Cell. 1992;71:343–353.
rosiglitazone. The exaggerated injury response in the WD
11. Zavaroni I, Sander S, Scott S, et al. Effect of fructose feeding on insulin
group is most likely a result of an interaction of these
secretion and insulin action in the rat. Metabolism. 1980;29:970 –973.
12. Hwang IS, Ho H, Hoffman BB, et al. Fructose-induced insulin resistance
abnormal metabolic factors and inflammation seen on this
and hypertension in rats. Hypertension. 1987;10:512–516.
diet in the apoE⫺/⫺ mouse.
13. Cantafora A, Bravo E, Yan CC. Characterization of lipoprotein fractions
The development of diabetes on a WD was recently
isolated from plasma of male Wistar rats by gradient ultracentrifugation.
described in the LDL receptor– deficient (LDLR⫺/⫺) mouse.
Proc Soc Exp Biol Med. 1993;204:90 –96.
14. Lai HC, Lasekan JB, Monsma CC, et al. Alteration of plasma lipids in the
However, there was no increase in spontaneous atherosclero-
rat by fractionation of modified milk fat (butterfat). J Dairy Sci. 1995;
sis in the aorta compared with LDLR⫺/⫺ mice on a FD.35 In
78:794 – 803.
Phillips et al
Type 2 Diabetes Mellitus in apoEⴚ/ⴚ Mice
15. Cerasi E, Luft R. Insulin response to glucose infusion in diabetic and
density lipoprotein receptor-deficient mice. Arterioscler Thromb Vasc
non-diabetic monozygotic twin pairs: genetic control of insulin response?
Acta Endocrinol (Copenh). 1967;55:330 –345.
26. Li AC, Brown KK, Silvestre MJ, et al. Peroxisome proliferator-activated
16. Grodsky GM, Curry D, Landahl H, et al. Further studies on the dynamic
receptor gamma ligands inhibit development of atherosclerosis in LDL
aspects of insulin release in vitro with evidence for a two-compartmental
receptor-deficient mice. J Clin Invest. 2000;106:523–531.
storage system [in Spanish]. Acta Diabetol Lat. 1969;6(suppl
27. Aizawa Y, Kawabe J, Hasebe N, et al. Pioglitazone enhances cytokine-
1):554 –578.
induced apoptosis in vascular smooth muscle cells and reduces intimal
17. Lacy PE, Walker MM, Fink CJ. Perifusion of isolated rat islets in vitro:
hyperplasia. Circulation. 2001;104:455– 460.
participation of the microtubular system in the biphasic release of insulin.
28. Lindner V, Fingerle J, Reidy MA. Mouse model of arterial injury. Circ
18. Marx N, Schonbeck U, Lazar MA, et al. Peroxisome proliferator-acti-
29. Manka D, Collins RG, Ley K, et al. Absence of p-selectin, but not
vated receptor gamma activators inhibit gene expression and migration in
intercellular adhesion molecule-1, attenuates neointimal growth after ar-
human vascular smooth muscle cells. Circ Res. 1998;83:1097–1103.
terial injury in apolipoprotein e-deficient mice. Circulation. 2001;103:
19. Ricote M, Huang J, Fajas L, et al. Expression of the peroxisome
1000 –1005.
proliferator-activated receptor gamma (PPARgamma) in human athero-
30. Phillips JW, Barringhaus KG, Sanders JM, et al. Single injection of
sclerosis and regulation in macrophages by colony stimulating factors and
P-selectin or P-selectin glycoprotein ligand-1 monoclonal antibody
oxidized low density lipoprotein. Proc Natl Acad Sci U S A. 1998;95:
blocks neointima formation after arterial injury in apolipoprotein
7614 –7619.
E-deficient mice. Circulation. 2003;107:2244 –2249.
20. Ricote M, Li AC, Willson TM, et al. The peroxisome proliferator-acti-
31. Movat H. Demonstration of all connective tissue elements in a single
vated receptor-gamma is a negative regulator of macrophage activation.
section. Arch Pathol Med. 1955;60:289 –295.
Nature. 1998;391:79 – 82.
32. Liu M, Shapiro ME. A new method for isolation of murine islets with
21. Ricote M, Welch JS, Glass CK. Regulation of macrophage gene
markedly improved yields. Transplant Proc. 1995;27:3208 –3210.
expression by the peroxisome proliferator-activated receptor-gamma.
33. Gotoh M, Maki T, Kiyoizumi T, et al. An improved method for isolation
Horm Res. 2000;54:275–280.
of mouse pancreatic islets. Transplantation. 1985;40:437– 438.
22. Law RE, Goetze S, Xi XP, et al. Expression and function of PPARgamma
34. Takagi T, Akasaka T, Yamamuro A, et al. Troglitazone reduces neointi-
in rat and human vascular smooth muscle cells. Circulation. 2000;101:
mal tissue proliferation after coronary stent implantation in patients with
non-insulin dependent diabetes mellitus: a serial intravascular ultrasound
23. Jackson SM, Parhami F, Xi XP, et al. Peroxisome proliferator-activated
study. J Am Coll Cardiol. 2000;36:1529 –1535.
receptor activators target human endothelial cells to inhibit leukocyte-en-
35. Merat S, Casanada F, Sutphin M, et al. Western-type diets induce insulin
dothelial cell interaction. Arterioscler Thromb Vasc Biol. 1999;19:
resistance and hyperinsulinemia in LDL receptor-deficient mice but do
2094 –2104.
not increase aortic atherosclerosis compared with normoinsulinemic mice
24. Xin X, Yang S, Kowalski J, et al. Peroxisome proliferator-activated
in which similar plasma cholesterol levels are achieved by a fructose-rich
receptor gamma ligands are potent inhibitors of angiogenesis in vitro and
diet. Arterioscler Thromb Vasc Biol. 1999;19:1223–1230.
in vivo. J Biol Chem. 1999;274:9116 –9121.
36. Kuhel DG, Zhu B, Witte DP, et al. Distinction in genetic determinants for
25. Collins AR, Meehan WP, Kintscher U, et al. Troglitazone inhibits for-
injury-induced neointimal hyperplasia and diet-induced atherosclerosis in
mation of early atherosclerotic lesions in diabetic and nondiabetic low
inbred mice. Arterioscler Thromb Vasc Biol. 2002;22:955–960.
Source: http://ley-lab.liai.org/publications/223.pdf
BD BBL™ Mueller Hinton Agar with 5% Sheep Blood 111-251801-N-00, December 2014 QUALITY CONTROL PROCEDURES BBLTM Muel er Hinton Agar with 5% Sheep Blood is recommended for disc diffusion susceptibility testing of Streptococcus pneumoniae with selected agents; i.e., chloramphenicol, erythromycin, ofloxacin, tetracycline and vancomycin, in addition to oxacil in screening for susceptibility to penicil in, as standardized by the Clinical and Laboratory Standards Institute (CLSI), formerly the National Committee for Clinical Laboratory Standards (NCCLS).
BMJ 2015;350:h231 doi: 10.1136/bmj.h231 (Published 11 February 2015) Sugar: spinning a web of influence Public health scientists are involved with the food companies being blamed for the obesity crisis,reports Jonathan Gornall Jonathan Gornall freelance journalist, Suffolk, UK An investigation by The BMJ has uncovered evidence of the