Levitra enthält Vardenafil, das eine kürzere Wirkdauer als Tadalafil hat, dafür aber schnell einsetzt. Männer, die diskret bestellen möchten, suchen häufig nach levitra kaufen ohne rezept. Dabei spielt die rechtliche Lage in der Schweiz eine wichtige Rolle.
Profiledental.gr


MINIMALLY INVASIVE ANTRAL MEMBRANE BALLOON ELEVATION • MAZOR ET AL
Flapless Approach to Maxillary Sinus
Augmentation Using Minimally Invasive
Antral Membrane Balloon Elevation
Ziv Mazor, DMD,* Efraim Kfir, DMD,† Adi Lorean, DMD,‡ Eitan Mijiritsky, DMD,§ and Robert A. Horowitz, DDS储
Posteriormaxillaryimplantplace- In the atrophic posterior max- floor. The surgical procedure was
ment is often complicated by the
illa, successful implant placement is
performed using a flapless ap-
lack of quality and volume of
often complicated by the lack of
proach. At 18 months follow-up, the
available bone. Types 3 and 4 bone
quality and volume of available
implant survival rate was 100%. Ab-
tend to predominate in the posterior
bone. In these cases, sinus floor aug-
sence of patient morbidity and satis-
maxilla, generally exhibiting the least
mentation is recommended to gain su-
factory bone augmentation with this
dense bone of the oral anatomy.1 The
fficient bone around the implants.
minimally invasive procedure sug-
height and width of the residual ridgecan significantly be reduced or elimi-
Sinus elevation can be performed by
gests that minimally invasive antral
nated by postextraction resorption pat-
either an open lateral window ap-
membrane balloon elevation should
terns, use of a removable prosthesis,
proach or by a closed osteotome ap-
be considered as an alternative to
physical trauma, periodontal disease,
proach depending on available bone
some of the currently used methods
and pneumatization of the sinus. In the
height. This case series demon-
of maxillary bone augmentation.
atrophic posterior maxilla, longer and
strates the feasibility and safety of
(Implant Dent 2011;20:434 – 438)
wider implants are needed to enhance
minimally invasive antral membrane
Key Words: antral membrane, pos-
long-term survival. This often requires
balloon elevation, followed by bone
terior maxillary implants, bone
bone augmentation beneath the sinus
augmentation and implant fixation
augmentation, dental implants,
to increase the vertical bone height.
in 20 patients with a residual bone
Tatum2 was the first to report the
height of 2 to 6 mm below the sinus
subantral augmentation or "sinus lift"procedure, which has evolved over thepast 25 years. A lateral window (mod-
the window is gently pressed inward
lary window offers an average implant
ified Caldwell-Luc) approach to the
and upward into the sinus cavity,
survival rate of 91.8% (range, 61.7%–
maxillary sinus is used. Because this
which lifts the Schneiderian mem-
100%)6 but involves potential compli-
has shown favorable results, the pos-
brane and serves as a new sinus floor.
cations (membrane tear, bleeding,
terior maxilla is often considered one
The void between the elevated tissues
infection, and sinus obstruction),
of the most predictable regions for
and the original sinus floor is filled
swelling and discomfort, and relative
grafting before or simultaneously with
with bone graft material. Implants
contraindications (sinus convolution
implant placement.2–7 Basically, a
may be simultaneously placed or the
septum or narrow sinus and previous
hinged window is created in the lateral
graft may be allowed to heal before
sinus surgery). Considerable surgical
wall of the maxilla.8 When completed,
implant placement.9–12
skills, equipment, and time are also
The "osteotome technique,"13 also
required. A modification of the
*Private Practice, Ra'anana, Israel.
called bone-added osteotome sinus
BAOSFE method is the minimally in-
†Private Practice, Petach Tikva, Israel.
‡Private Practice, Tiberias, Israel.
floor elevation (BAOSFE), is an alter-
vasive antral membrane balloon eleva-
§Private Practice, Tel Aviv, Israel.
储Assistant Clinical Professor, Departments of Periodontics and
native approach for sinus elevation
tion (MIAMBE). Antral membrane
Implantology, Oral Surgery, New York College of Dentistry, NY.
where a small amount of bone height
elevation is performed through the os-
Reprint requests and correspondence to: Ziv Mazor,
is missing. It is not suitable for pa-
teotomy site (ⱕ3.5 mm) using a spe-
DMD, 142 Ahuza Street, Ra'anana 43300, Israel,
tients with markedly reduced initial
cially designed balloon. The use of
Phone: 972-97400336, Fax: 972-97602839, E-mail:
[email protected]
bone height.14 BAOSFE can be com-
this technique as an alternative to con-
plicated by membrane perforation and
ISSN 1056-6163/11/02006-434Implant Dentistry
tear,15 which can be reduced with ex-
Volume 20 • Number 6
Copyright 2011 by Lippincott Williams & Wilkins
pert technique and specially designed
Advantages of using a flapless ap-
instrumentation.16 The lateral maxil-
proach for dental implant placement

IMPLANT DENTISTRY / VOLUME 20, NUMBER 6 2011
are well known21–27— demonstratingpredictability, preservation of crestalbone and mucosal health surroundingthe implants. A flapless approach com-bined with MIAMBE has never beendescribed. In this study, a MIAMBEballoon-harboring device (MiambeLTD, Netanya, Israel) was used. This isa stainless steel tube, 3 mm in diameter,that connects on its proximal end to thededicated inflation syringe and on its
Fig. 3. Underlying bony crest exposed using
distal portion has an embedded single-
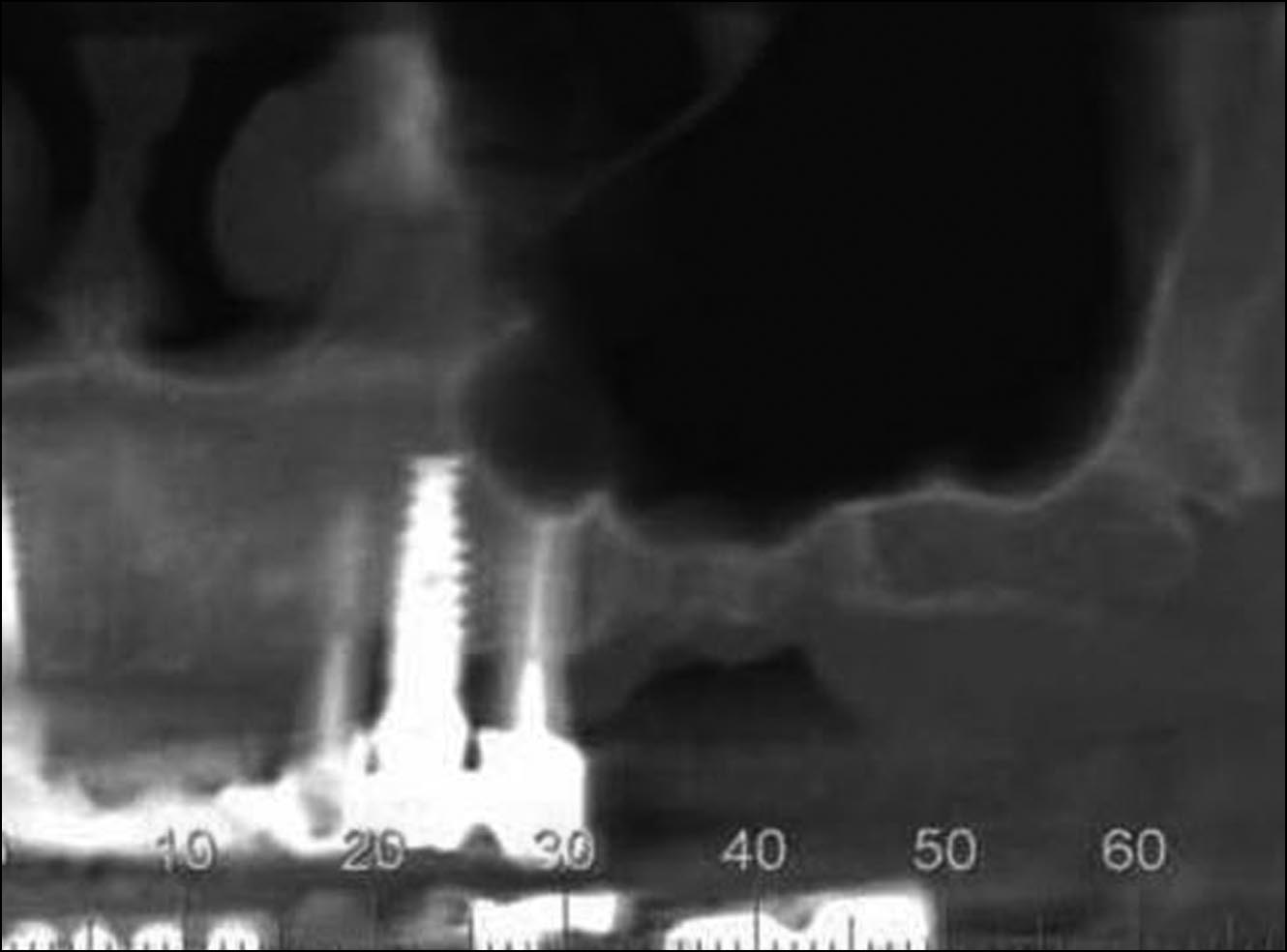
Fig. 1. Panoramic projection of the residual
ridge underneath the sinus floor.
a 4 mm punch.
use silicone balloon. The balloon is in-flated with diluted contrast fluid thatpushes up the Schneiderian membrane,creating the desired height for implantplacement.
The purpose of this study was to
describe a case series using this newtreatment modality with its advantagesthrough a flapless approach with 18months follow-up.
MATERIALS AND METHODS
Patient Selection
All patients were from the au-
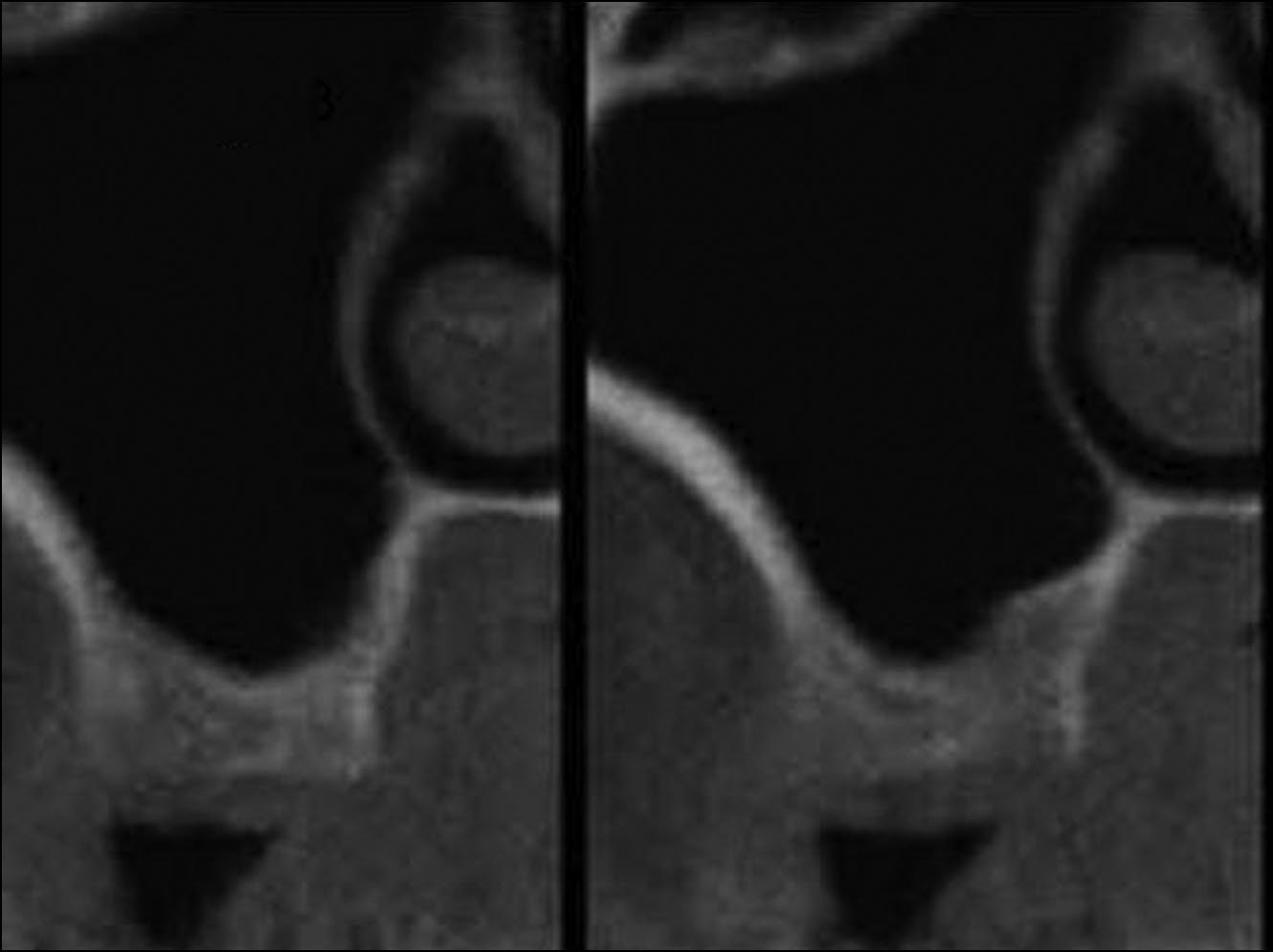
Fig. 2. CBCT axial cuts of the residual ridge
Fig. 4. Osteotomy preparation using the Pi-
thors' private practices, selected after
underneath the sinus floor demonstrating
ezosurgery device.
meticulous evaluation of their medical
3– 4 mm of alveolar bone height.
histories and dental examinations, in-cluding panoramic radiographs anddental cone beam CT (CBCT) scans.
Local anesthesia (infiltration of
The mucosa thickness and pathology,
posterior and middle superior alveolar
bone height and thickness, sinus struc-
nerve and greater palatine nerve) was
ture, and major blood vessels were
administered using 2% lidocaine (No-
assessed. Patients received an oral ex-
vocol Pharmaceutical Inc., Cam-
planation regarding the procedure and
bridge, Ontario, Canada). To obtain
signed an informed consent. A prereq-
platelet-rich fibrin (PRF), 40 mL of
uisite included crestal bone height of 2
blood was drawn by venous puncture
to 6 mm between the sinus floor and
and processed. Under local anesthesia,
the alveolar ridge. In 20 patients, rang-
a 4-mm diameter punch was used to
ing in age from 37 to 72 years (mean,
remove the epithelium with connec-
Fig. 5. The metal sleeve of the balloon-
49 years), a total of 24 sinuses were
tive tissue and to expose the underlin-
harboring device inserted into the mesial os-
treated and 37 screw-type endosseous
ing bone crest at the precise future
teotomy, 1 mm beyond the sinus floor.
implants inserted. All patients were
implant location (Fig. 3).
treated under local anesthesia in the
An ultrasonic Piezoelectric (Mec-
dental office.
tron S.P.A, Genova, Italy) round dia-
MIAMBE osteotome. After removing
mond tip drill was used in the center of
the osteotome, the membrane integrity
the exposed alveolar crest up to 1 to 2
was assessed by Valsalva maneuver.
The exact bone height between the
mm below the sinus floor. Depth was
The metal sleeve of the balloon-
alveolar crest and the sinus floor was
predetermined according to measure-
harboring device (Miambe LTD),
assessed using preoperative CBCT
ments obtained from the CT scan and
specifically designed for sinus aug-
scans (Figs. 1 and 2). A preprocedural
periapical radiographs. The ultrasonic
mentation procedures, was inserted
nonsteroidal anti-inflammatory agent,
diamond insert was used to deepen the
into the osteotomy 1 mm beyond the
Augmentin (GlaxoSmith Kline, Brent-
osteotomy until the sinus membrane
sinus floor (controlled by Teflon stop-
ford Middlesex, United Kingdom) (cla-
was reached (Fig. 4). Bone graft ma-
per) (Figs. 5– 8). The balloon was
vulanate potassium), 875 mg, was
terial and PRF were inserted into the
slowly inflated with the barometric in-
administered twice, 24 hours before
osteotomy, subsequently enlarging the
flator up to 2 atm. Once the balloon
osteotomy from 2 to 2.9 mm with the
emerged from the metal sleeve under

MINIMALLY INVASIVE ANTRAL MEMBRANE BALLOON ELEVATION • MAZOR ET AL
Fig. 9. A mixture of xenograft grafting mate-
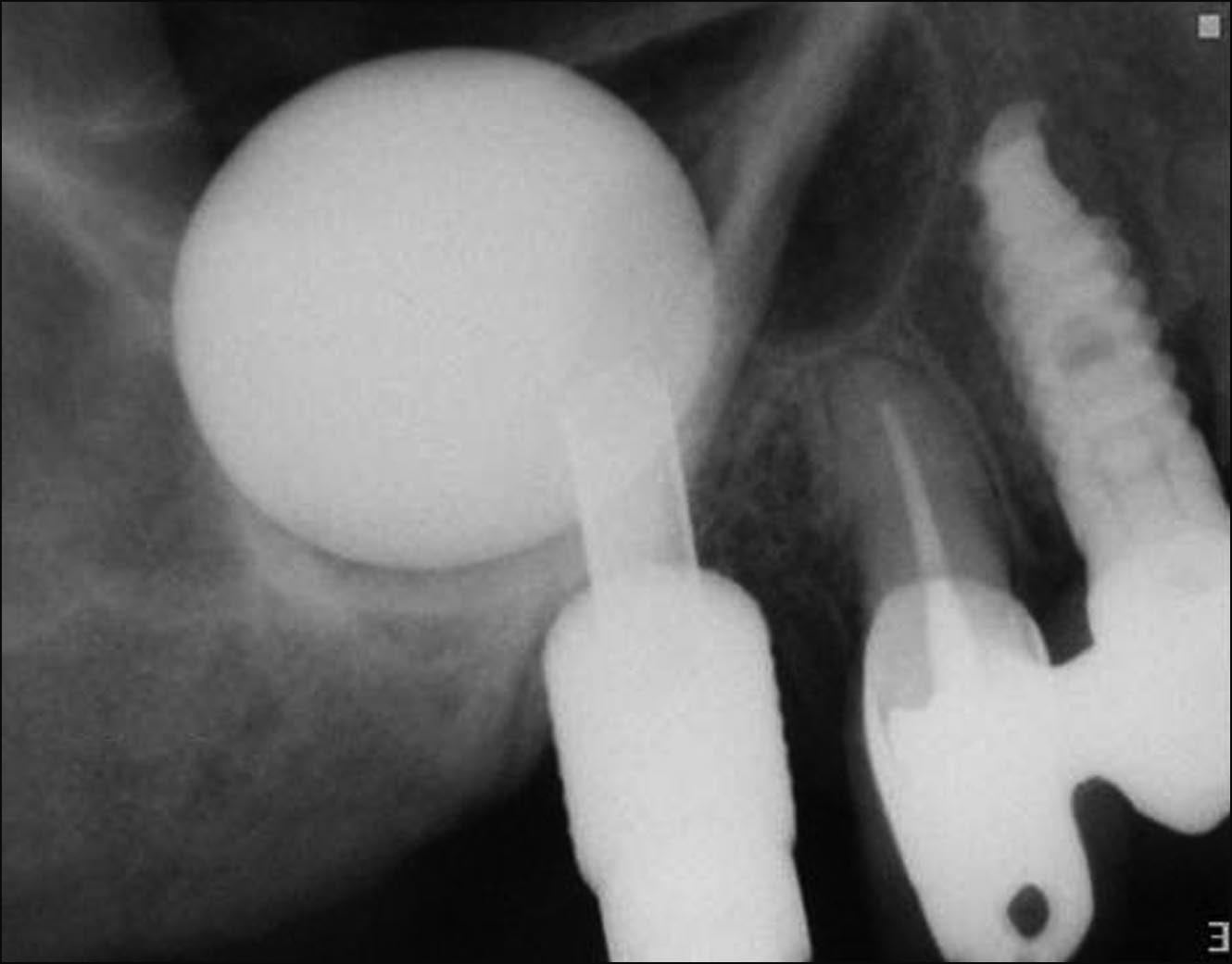
Fig. 6. Periapical radiograph demonstrating
rial ⫹ PRF is injected to the osteotomy sites
Fig. 12. Periapical radiograph 6 months
balloon inflation in mesial site.
after balloon removal.
10). The healing abutment was con-nected to the inserted implants and aperiapical radiograph verified implantand graft positions (Fig. 11).
Patients were discharged with ibu-
profen, 600 mg (single dose) for painrelief and Augmentin, 875 mg twicedaily for 7 days. At 6 months postsur-gery, patients were evaluated radio-graphically (panoramic and periapical)
Fig. 7. The metal sleeve of the balloon-
Fig. 10. Self-threading implants, 5 mm in di-
before implant exposure. Clinical crite-
harboring device inserted into the distal os-
ameter and 13 mm long, inserted into theosteotomy sites.
ria at the time of implant exposure in-
teotomy, 1 mm beyond the sinus floor.
cluded stability in all directions, crestalbone resorption, and any reported painor discomfort. Prosthetic rehabilitationwas initiated 3 weeks after implant ex-posure. Patients were monitored andfollowed-up for 18 months (Fig. 12).
All patients received the MIAMBE
treatment with immediate implantplacement. Healing was uneventful,with no symptoms of pain or edema,
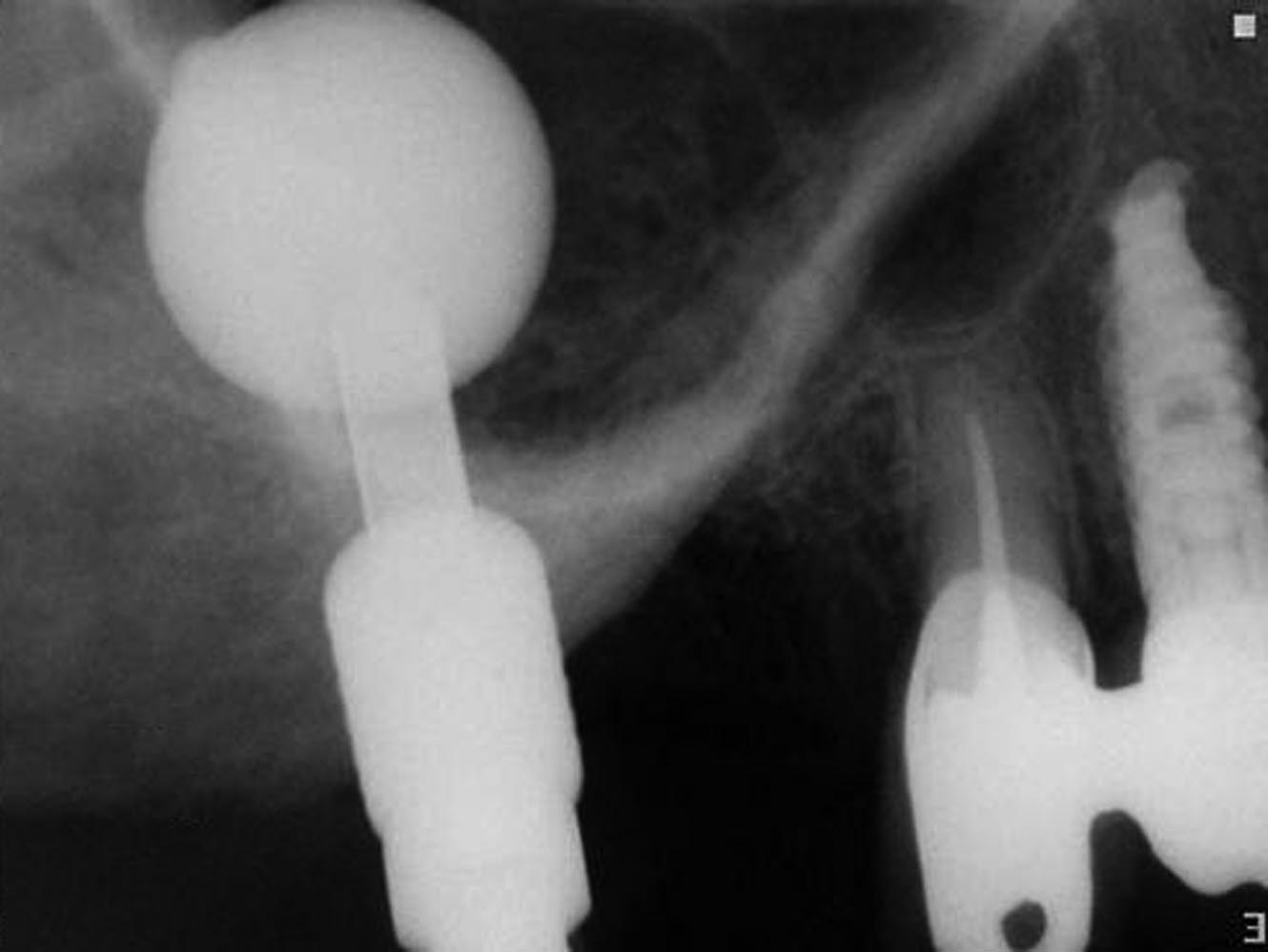
Fig. 8. Periapical radiograph showing balloon
inflation in the distal site.
Fig. 11. Healing abutments screwed into
postsurgery. One patient, who was al-
lergic to the antibiotic Augmentin(GlaxoSmith Kline, Brentford Middle-
the sinus membrane, the pressure
then deflated and removed. Membrane
sex, United Kingdom), was prescribed
dropped to 0.5 atm. Subsequently, the
integrity was assessed by Valsalva ma-
Clindamycin (Pfizer Pharmaceuticals,
balloon was inflated with a progres-
neuver and direct visualization assisted
Poce Sur Cisse, France).
sively higher volume of contrast fluid.
by applying a small suction tip.
At 1 week postsurgery, patients
The same procedure was applied to the
A bone graft injector was filled
were recalled and consequently fol-
second osteotomy site.
with a mixture of bone substitute
lowed up for 6 months. At 6 months,
Periapical radiographs were taken
(Cerabone-Botiss, Berlin, Germany) ⫹
all implants were successfully inte-
to evaluate balloon inflation and mem-
PRF and injected through the osteot-
grated. Implants were restored with
brane elevation. After the desired ele-
omy into the sinus under the antral
porcelain fused to metal crowns and
vation (11 mm) was obtained, the
membrane (Fig. 9). Screw-type im-
followed-up for 18 months. The cr-
balloon remained inflated in the sinus
plants (Adin Touareg-Alon Tavor,
estal bone height was maintained and
for 5 minutes to reduce the sinus mem-
Afula, Israel), 13 mm in length and 5
verified by subsequent radiographs.
brane elasticity. The balloon was
mm in diameter, were inserted (Fig.
No adverse effects were noted.
IMPLANT DENTISTRY / VOLUME 20, NUMBER 6 2011
Dr. Efraim Kfir claims to be a Board
neous implant placement in the severely
Member and a consultant for Miambe
atrophic maxilla. J Periodontol. 1998;69:
This case series supports the prop-
LTD. Dr. Adi Lorean claims to have
osition that MIAMBE is a minimally
13. Summers RB. Sinus floor elevation
had, in the past, "administrative sup-
invasive, single-sitting procedure of
with osteotomes. J Esthet Dent. 1998;10:
port." The other authors claim to have
maxillary bone augmentation, and im-
no financial interest, either directly or
plant placement can be performed
14. Nkenke E, Schlegel A, Schultze-
indirectly, in any of the products or
where previous conventional lateral
Mosgau S, et al. The endoscopically con-
companies mentioned in this article.
trolled osteotome sinus floor elevation: A
window sinus augmentation had been
preliminary prospective study. Int J Oral
Maxillofac Implants. 2002;17:557-566.
The "osteotome technique"
15. Berengo M, Sivolella S, Majzoub Z,
(BAOSFE) is minimally invasive.
1. Truhlar RS, Orenstein IH, Morris HF,
et al. Endoscopic evaluation of the bone-
However, if the initial height is ⱕ4
et al. Distribution of bone quality in patients
added osteotome sinus floor elevation pro-
mm, this method is clearly inferior to
receiving endosseous dental implants.
cedure. Int J Oral Maxillofac Surg. 2004;
the lateral window approach.28 The
J Oral Maxillofac Surg. 1997;55(suppl 5):
BAOSFE yields modest antral mem-
16. Toffler M. Staged sinus augmenta-
2. Tatum H Jr. Maxillary and sinus im-
tion using a crestal core elevation proce-
brane elevation and bone augmenta-
plant reconstructions. Dent Clin North Am.
dure and modified osteotomes to minimize
tion, requires considerable skills, and
membrane perforation. Pract Proced Aes-
may frequently result in membrane
3. Boyne PJ, James RA. Grafting of the
thet Dent. 2002;14:767-774.
tear, even when selectively applied29
maxillary sinus floor with autogenous mar-
17. Kfir E, Kfir V, Mijiritsky E, et al. Min-
and endoscopically controlled. The
row and bone. J Oral Surg. 1980;38:613-
imally invasive antral membrane balloon
use of the specific dedicated Miambe
elevation followed by maxillary bone aug-
4. Misch CE. Maxillary sinus augmen-
balloon enables the operator to pre-
mentation and implant fixation. J Oral Im-
tation for endosteal implants: Organized
dictably elevate the Schneiderian
alternative treatment plans. Int J Oral Im-
18. Kfir E, Kfir V, Eliav E, et al. Minimally
membrane and place implants that are
13-mm long. The successful use of the
5. Block MS, Kent JN, Kallukaran FU,
elevation: Report of 36 procedures. J Peri-
flapless approach actually requires ad-
et al. Bone maintenance 5 to 10 years after
vanced clinical experience and surgi-
sinus grafting. J Oral Maxillofac Surg.
19. Kfir E, Goldstein M, Rafaelov R, et
cal judgment. The flapless approach
al. Minimally invasive antral membrane bal-
6. Wallace SS, Froum SJ. Effect of
together with the MIAMBE used in
loon elevation in the presence of antral
maxillary sinus augmentation on the sur-
this study has several advantages over
septa: A report of 26 procedures. J Oral
vival of endosseous dental implants. A sys-
the lateral window approach and the
tematic review. Ann Periodontol. 2003;8:
20. Kfir E, Goldstein M, Yerushalmi I, et
BAOSFE techniques. These include
al. Minimally invasive antral membrane bal-
reduced patient trauma, improved pa-
7. Peleg M, Garg AK, Mazor Z. Predict-
loon elevation—Results of a multicenter
tient comfort and recuperation, de-
ability of simultaneous implant placement
registry. Clin Implant Dent Relat Res. 2009;
in the severely atrophic posterior maxilla: A
creased surgical time, faster soft tissue
9-year longitudinal experience study of
healing, and normal oral hygiene pro-
21. Campelo LD, Camara JR. Flapless
2132 implants placed into 731 human si-
cedures immediately postsurgery.23–25
implant surgery: A 10-year clinical retro-
nus grafts. Int J Oral Maxillofac Implants.
The use of preoperative CBCT mea-
spective analysis. Int J Oral Maxillofac Im-
surements and direct visualization of
8. Friberg B, Nilson H, Olsson M, et al.
22. Becker W, Goldstein M, Becker B,
the sinus membrane through the spe-
MkII: The self-tapping Brånemark implant:
et al. Minimally invasive flapless implant
cifically designed suction tip, as well
5-year results of a prospective 3-centerstudy. Clin Oral Implant Res. 1997;8:279-
surgery: A prospective multicenter study.
as illumination, can overcome the dis-
Clin Implant Dent Relat Res. 2005;7:
ability to directly visualize the sinus
9. Froum SJ, Tarnow DP, Wallace SS,
compartment as seen in the open lat-
et al. Sinus floor elevation using anorganic
23. Rousseau P. Flapless and tradi-
eral window approach.
bovine bone matrix (OstoGraf/N) with and
tional dental implant surgery: An open,
without autogenous bone: A clinical, histo-
retrospective comparative study. J OralMaxillofac Surg. 2010;68:2299-2306.
logic, radiographic, and histomorphomet-
ric analysis—Part 2 of an ongoing study.
24. Noelken R, Kunkel M, Wagner W.
When the advantages of flapless
Int J Periodontics Restorative Dent. 1998;
Immediate implant placement and provi-
surgery are combined with MIAMBE,
sionalization after long-axis root fractureand complete loss of the facial bony la-
the surgeon is able to perform a pro-
10. Peleg M, Chaushu G, Mazor Z, et
al. Radiological findings of the post-sinus
mella. Int J Periodontics Restorative Dent.
cedure with minimal postoperative
lift maxillary sinus: A computerized tomog-
symptoms as well as reduced chair
raphy follow-up. J Periodontol. 1999;70:
25. Ravindran DM, Sudhakar U, Ra-
makrishnan T, et al. The efficacy of flapless
11. Smiler DG. The sinus lift graft: Ba-
implant surgery on soft-tissue profile
sic technique and variations. Pract Perio-
comparing immediate loading implants
dontics Aesthet Dent. 1997;9:885-893.
to delayed loading implants: A compara-
Dr. Ziv Mazor claims to be a con-
12. Peleg M, Mazor Z, Chaushu G, et
tive clinical study. J Indian Soc Periodon-
sultant for Adin Implants, Miambe.
al. Sinus floor augmentation with simulta-
MINIMALLY INVASIVE ANTRAL MEMBRANE BALLOON ELEVATION • MAZOR ET AL
26. Bayounis AM, Alzoman HA, Jan-
verely resorbed maxilla—A 5-year clinical
consecutively treated patients. Int J
sen JA, et al. Healing of peri-implant tis-
study. Int J Periodontics Restorative Dent.
Oral Maxillofac Implants. 1999;14:853-
sues after flapless and flapped implant
installation. J Clin Periodontol. 2011;38:
28. Rosen PS, Summers R, Mella-
29. Fugazzotto PA. Augmentation of
do JR, et al. The bone-added osteo-
the posterior maxilla: A proposed hierarchy
27. Barter S. Computer-aided implant
tome sinus floor elevation technique:
of treatment selection. J Periodontol.
placement in the reconstruction of a se-
Multicenter retrospective report of
Source: http://www.profiledental.gr/wp-content/uploads/2015/02/FlaplessApproachToMaxillarySinusAugmentationUsingMinimallyInvasiveAntralMembraneBalloonElevation2.pdf
Hyperbaric oxygen treatment for haemorrhagic radiation materais ana metnOas Radiation-induced severe haemorrhagic cystitis is difficult January, 1986, until January, 1994, 40 patients with severe haemorrhagic radiation-induced cystitis were treated with HBO. Inclusion criteria were severe haemorrhagic cystitis due to haematuria but do not affect the radiocystitis itself.
TENBY SCHOOLS MALAYSIA APPLICATION FOR ADMISSION CHECKLIST Before submitting the Admissions Form to the specific school in Tenby Schools Group, please check that all documentation listed below has been attached to ensure smooth processing. 1. Application for Admission Form Please complete the Admissions Form. All sections must be completed.