Levitra enthält Vardenafil, das eine kürzere Wirkdauer als Tadalafil hat, dafür aber schnell einsetzt. Männer, die diskret bestellen möchten, suchen häufig nach levitra kaufen ohne rezept. Dabei spielt die rechtliche Lage in der Schweiz eine wichtige Rolle.
Drug-induced liver injury following a repeated course of ketamine treatment for chronic pain in crps type 1 patients: a report of 3 cases
PAINÒ 152 (2011) 2173–2178
Drug-induced liver injury following a repeated course of ketamine treatmentfor chronic pain in CRPS type 1 patients: A report of 3 cases
Ingeborg M. Noppers Marieke Niesters Leon P.H.J. Aarts Martin C.R. Bauer Asbjørn M. Drewes Albert Dahan , Elise Y. Sarton
a Department of Anesthesiology, Leiden University Medical Center, Leiden, The Netherlandsb Mech-Sense, Department of Gastroenterology and Hepatology, Aalborg Hospital, Aarhus University Hospital, 9000 Aalborg, Denmark
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Studies on the efficacy of ketamine in the treatment of chronic pain indicate that prolonged or repetitive
Received 18 October 2010
infusions are required to ensure prolonged pain relief. Few studies address ketamine-induced toxicity.
Received in revised form 20 March 2011
Here we present data on the occurrence of ketamine-induced liver injury during repeated administrations
Accepted 21 March 2011
of S(+)-ketamine for treatment of chronic pain in patients with complex regional pain syndrome type 1 aspart of a larger study exploring possible time frames for ketamine re-administration. Six patients werescheduled to receive 2 continuous intravenous 100-hour S(+)-ketamine infusions (infusion rate 10–
20 mg/h) separated by 16 days. Three of these patients developed hepatotoxicity. Patient A, a 65-year-
old woman, developed an itching rash and fever during her second exposure. Blood tests revealed elevated
Side effectsLiver injury
liver enzymes (alanine transaminase, alkaline phosphatase, aspartate transaminase, and c-glutamyl trans-
ferase, all P3 times the upper limit of normal) and modestly increased eosinophilic leukocytes. Patient E, a48-year-old woman, developed elevated liver enzymes of similar pattern as Patient A during her secondketamine administration and a weakly positive response to antinuclear antibodies. In a third patient,Patient F, a 46-year-old man, elevated liver enzymes (alanine transaminase and c-glutamyl transferase)were detected on the first day of his second exposure. In all patients, the ketamine infusion was promptlyterminated and the liver enzymes slowly returned to reference values within 2 months. Our data suggestan increased risk for development of ketamine-induced liver injury when the infusion is prolonged and/orrepeated within a short time frame. Regular measurements of liver function are therefore required duringsuch treatments.
Ó 2011 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
Most of the published randomized controlled trials (36/38) are ofpoor-to-moderate quality. Despite the absence of good quality
It is well established that the N-methyl-D-aspartate receptor
studies, ketamine treatment seems to get a definite place in the
(NMDAR) plays an important role in the etiology and duration of
treatment of chronic pain in clinical practice The use of keta-
chronic pain . Chronic pain activates and upregulates
mine has raised the concern for toxicity . Animal studies indi-
the NMDAR in the dorsal horn of the spinal cord, which causes en-
cate that ketamine use is associated with neurotoxicity and
hanced signal transmission in the pain circuitry and leads to
learning disabilities, while human studies indicate abuse potential
chronic pain, often coupled with allodynia and hyperalgesia
and a high frequency of psychotropic side effects. Case reports on
Consequently, drugs that block the NMDAR are able to re-
the side effects and toxicity of the recreational abuse of ketamine
lieve chronic pain and possibly modulate the underlying disease
indicate a pattern of renal and liver toxicity During the
process . The most potent NMDAR antagonist currently
course of a study on repeated administrations of ketamine for
available is ketamine, and the number of studies on the efficacy
treatment of chronic pain in patients with complex regional pain
of ketamine increases rapidly. Since 1992 there are 38 published
syndrome type 1 (CRPS), we encountered hepatotoxicity in a sub-
randomized controlled trials on ketamine use in chronic (noncan-
set of patients that received 2 100-hour infusions of S(+)-ketamine
cer) pain patients and even more open-label and case studies .
at a 16-day interval. Six subjects were enrolled in that study armand liver damage was observed in 3 of them. This prompted usto end the trial prematurely. Liver damage is considered a rare side
⇑ Corresponding author. Address: Department of Anesthesiology, Leiden Univer-
effect of ketamine use, but since repeated dosing is often neces-
sity Medical Center, P5-Q, 2300 RC Leiden, The Netherlands.
E-mail address: (A. Dahan).
sary, we believe that awareness of this side effect is needed. We
0304-3959/$36.00 Ó 2011 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
doi:
I.M. Noppers et al. / PAINÒ 152 (2011) 2173–2178
therefore present the course of events of the 6 subjects enrolled in
0–17 U/L], c-glutamyl transferase [cGT; reference values 5–40 U/
the 16-day interval study arm.
L]) were measured during ketamine treatment (in weeks 1 and4) on days 1 (before the start of drug infusion), 3, and 5. In case
of liver enzyme elevation, the frequency of testing increased totwice daily. Heart rate, blood pressure, and tympanic temperature
The patients presented were involved in a study registered in
were obtained 3 times per day.
the Netherlands Trial Register (under num-ber NTR1550. This pilot study was aimed at generating exploratory
data on the effect of two 5-day (i.e., 100 h) ketamine treatments(treatment 1 in week 1, treatment 2 in week 4) on pain relief in
The total number of subjects in this pilot study was arbitrarily
CRPS 1 patients.
set at 30 (10 per group). No comparative analysis was planned,and the data are presented in a descriptive manner only.
Patients eligible for the study were those referred to our outpa-
tient pain clinic and who were diagnosed with CRPS-1, as based on
Patient admissions took place between December 2008 and
the International Association for the Study of Pain CRPS-1 criteria
February 2010. The inclusion of patients in the study was ended
, and who had pain scores of 5 or higher (on a numerical rating
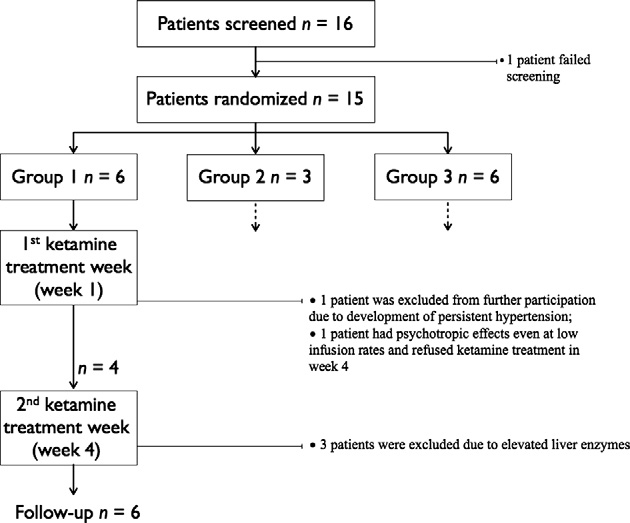
prematurely after 13 subjects had been admitted. Five of the 6 sub-
scale [NRS] from 0 to 10 where 0 = no pain and 10 = worst pain).
jects randomized to Group 1 developed side effects: one developed
Exclusion criteria included age <18 years, inability to give informed
severe hypertension and another psychotropic side effects during
consent, serious medical disease (e.g., cardiovascular, renal, or liver
their first exposure to S(+)-ketamine, and 3 developed elevated
disease), use of strong opioids or baclofen, pregnancy/lactation,
hepatotoxicity prior to or during their second exposure to S(+)-ket-
and history of psychosis. Patients were asked not to change their
amine. The development of hepatotoxicity was such that we
pain medication from the start of the study until completion of fol-
decided that continuation of the trial was unjustifiable. See
for a flow chart of the study. None of the subjects randomized toGroups 2 (n = 2) and 3 (n = 5) developed severe side effects. In
2.2. Trial design
, the characteristics of patients randomized to Group 1 aregiven.
The study design was single blind. Patients were admitted twice
for 5 days and randomly allocated to 1 of 3 groups: Group 1 was
3.1. Patient A: a 65-year-old woman with CRPS in her left foot
admitted in weeks 1 and 4 and received ketamine on both occa-sions (ie, they had a 16-day ketamine-free interlude); Groups 2
During treatment in week 1, pain score reduced from 7 to 2 on
and 3 were admitted in weeks 1 and 13 and received ketamine
day 2 of the ketamine infusion. Due to the development of severe
on both occasions (Group 2) or midazolam on the first occasion
psychotropic side effects, nausea, and dizziness, the infusion was
and ketamine on the second (Group 3). Follow-up was performed
reduced to 2.1 lg kg 1 h 1 on day 2. At this infusion rate, side ef-
during the 12 weeks after the second admission. Since the focus
fects were bearable. An increase in infusion rate was not possible,
of this report is on the side effects observed in the Group 1 subset
and the pain score increased to 5 at the end of the infusion. No in-
of patients, we restrict our presentation to these patients.
crease in liver enzymes was detected in treatment week 1 Upon admission in week 4, pain had returned to prestudy baseline
level and on day 2 of the treatment, similar side effects occurred ashad been seen in week 1 (ketamine infusion rate 2.7 lg kg 1 h 1,
S(+)-ketamine (Ketanest S, Pfizer BV, Capelle a/d IJssel, The
pain score 2). After 72 h of ketamine infusion, the patient devel-
Netherlands) was administered continuously by intravenous route
oped an itching rash on legs, abdomen, back, and upper arms,
for 5 days according to an infusion scheme of Sigtermans et al.
combined with an increase in tympanic temperature to 38.3 °C.
On day 1, infusion started at 8 am at 1.2 lg kg 1 h 1. Three times aday (at 8 am, noon, and 4 pm), the infusion rate could be increasedin steps of 0.6 lg kg 1 h 1 until a maximum infusion rate of7.2 lg kg 1 h 1 was reached. When the patient reached a painrating of zero, the infusion rate was not further changed. In caseof severe side effects, the infusion rate was lowered in steps of0.6 lg kg 1 h 1 and later increased again if possible. On day 5, atnoon, the infusion ended. In case of nausea, 10 mg oral domperi-done could be given, with a maximum of 40 mg per day.
2.4. Measurements
The primary outcome measure of the study was pain relief as
measured by the 10-point NRS ranging from 0 (no pain) to 10(worst pain), measured 3 times daily (8 am, 12 pm, and 4 pm)during treatment, and weekly in between treatments and duringfollow-up. Secondary outcome parameters were psychotropic sideeffects, nausea, and headache, all scored on a range from 0 (notpresent) to 10 (maximal presence). Liver enzymes (alkaline phos-phatase [ALP; reference values 40–120 U/L], alanine transaminase[ALT; reference values 5–34 U/L], aspartate transaminase [AST;reference values 5–30 U/L], total bilirubin [TBIL; reference values
Fig. 1. Flow chart of Group I of the study at the time of study termination.
I.M. Noppers et al. / PAINÒ 152 (2011) 2173–2178
Table 1Patient characteristics, NRS and ketamine treatment.
Patient Age (y); Sex BMI
Duration of Affected
Ketamine amount Ketamine amount
baseline in week 1
Tramadol 3 dd 50 mg
Paracetamol/codeine od
Both arms Ibuprofen 600 mg od
i.v. Line placement 144
Right arm Tramadol 3 dd 100 mg
Gabapentin 4 dd 600 mgIbuprofen 2 dd 800 mgOral contraceptive
Tramadol 1 dd 150 mg
tramadol/paracetamol 4 dd 325/37.5 mgAmitriptyline 1 dd 20 mg
Naproxen 2 dd 500 mg
Cannabis tea 1–2/wk
BMI, body mass index; CRPS, complex regional pain syndrome type 1; NRS, numerical rating scale; i.v., intravenous; od, on demand; dd, times daily.
The blood tests performed on day 3 revealed elevated liver en-
she experienced severe psychotropic side effects: fearsome halluci-
zymes (see ; ALP, ALT, AST, TBIL, and cGT exceeded the upper
nations and a panic attack. She refused further treatment and was
reference values). A diagnosis of drug-induced liver injury (DILI)
discharged with a pain score of 4. Pain relief lasted for another
was made and the ketamine infusion was terminated (total
13 weeks. No increase in liver enzymes was detected during keta-
amount of ketamine infused at that time was 1.3 g). Also, all other
mine treatment.
medication was stopped. Jaundice and tenderness or enlargementof the liver were absent on physical examination. No further abnor-
3.3. Patient C: A 39-year-old woman with CRPS in both arms
malities were observed in blood hematology or chemistry, apartfrom a small increase in eosinophilic and neutrophilic leukocytes
In treatment week 1 there was a slow and modest reduction in
(to 8% and 77%, respectively). The patient received topical cortico-
CRPS pain score from 9 to 6 on day 3. She developed a gradual in-
steroid and oral clemastine to treat the pruritis. Liver enzymes de-
crease in mean arterial blood pressure from 93 to 135 mm Hg on
creased upon termination of the ketamine infusion, except for ALP
day 3. Decreasing the infusion rate did not lower the blood pres-
and cGT, which increased for another day. The patient was dis-
sure and the treatment was terminated on day 4 (pain score 6,
charged on day 5 with an NRS of 3. After discharge the rash slowly
mean arterial pressure 130 mm Hg). The decision was made by
improved, disappearing completely within 2 weeks. Liver enzymes
the investigators and patient to not participate in the second keta-
returned to normal within 1 month, except for cGT, which normal-
mine session. The high blood pressure was successfully treated
ized within 2 months. The patient continued to experience a lack of
with antihypertensive medication that is continued to date. No in-
energy following discharge for 6 months. The pain score returned
crease in liver enzymes was detected during ketamine treatment.
to baseline 5 weeks after discharge.
3.4. Patient D: A 20-year-old woman with CRPS of the left leg
3.2. Patient B: A 53-year-old woman with CRPS in her right arm
Upon admission in week 1, CRPS pain score was 9. The ketamine
Ketamine produced a reduction in CRPS pain score from 8 to 2
infusion rate was increased to the maximum dose without any
on treatment day 2. On day 3 the patient was pain free. On day 4
effect on the pain score. The patient experienced no side effects.
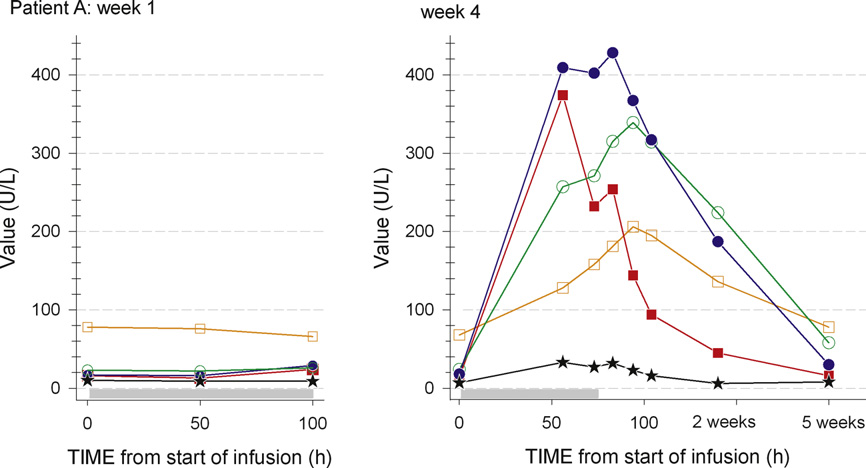
Fig. 2. Serum liver enzymes in the first (left) and second (right) S(+)-ketamine treatment week (= study week 4) of patient A. Alkaline phosphatase, alanine transaminase,aspartate transaminase, total bilirubin, and c-glutamyl transferase exceeded the upper reference values. Reference values: alkaline phosphatase (orange open square) 40–120 U/L, alanine transaminase (blue closed circle) 5–34 U/L, aspartate transaminase (red closed square) 5–30 U/L, total bilirubin (black star) 0–17 U/L, and c-glutamyltransferase (green open circle) 5–40 U/L. The gray bar indicates the ketamine infusion.
I.M. Noppers et al. / PAINÒ 152 (2011) 2173–2178
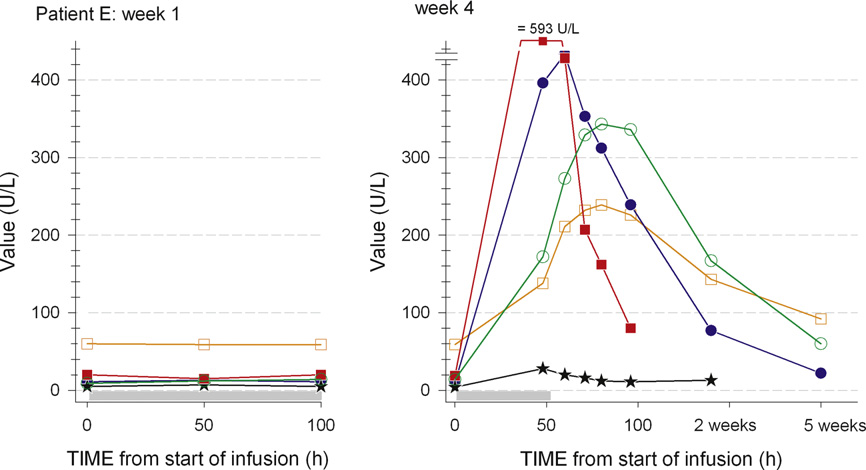
Fig. 3. Serum liver enzymes in the first (left) and second (right) S(+)-ketamine treatment week (= study week 4) of patient E. Alkaline phosphatase, alanine transaminase,aspartate transaminase, total bilirubin, and c-glutamyl transferase exceeded the upper reference values (for reference values see legend). The gray bar indicates theketamine infusion.
On day 5 the patient was discharged with pain score 9. A similar
terminated on the same day after 6 h of infusion, when the results
course was observed during treatment in week 4. The pain score
of the blood screening became available: ALT was elevated to 77
was 9 upon discharge and remained between 8 and 9 during the
U/L (normal range 5–34 U/L) and cGT was elevated to 267 U/L
follow-up period. No increase in any of the liver enzymes was de-
(5–40 U/L). The other enzymes remained within the range of normal.
tected during ketamine treatment in weeks 1 and 4.
A second sample 8 h after the initiation of treatment gave similarvalues. The patient denied the use of alcohol, intake of any medica-
3.5. Patient E: a 48-year-old woman with CRPS of the right foot
tion, or any episodes of epigastric pain in the period prior to hissecond admission. Blood hematology tests revealed the absence of
Ketamine induced gradual pain relief, with CRPS pain NRS 6 to 0
gallstones or signs of infection. Since we discontinued ketamine
on day 4. During treatment the patient experienced various side
treatment, the patient refused any follow-up blood measurements.
effects, including psychotropic effects, sedation, dizziness, and
Two additional blood samples were taken 1 week and 4 months
nausea. No increase in liver enzymes was detected during the first
later, by the patient's family doctor: cGT remained elevated
ketamine treatment week. Upon the start of treatment in week 4,
(92 U/L) in the first sample but was normalized in the second.
CRPS pain score was 3. Within 1 day of ketamine treatment, the
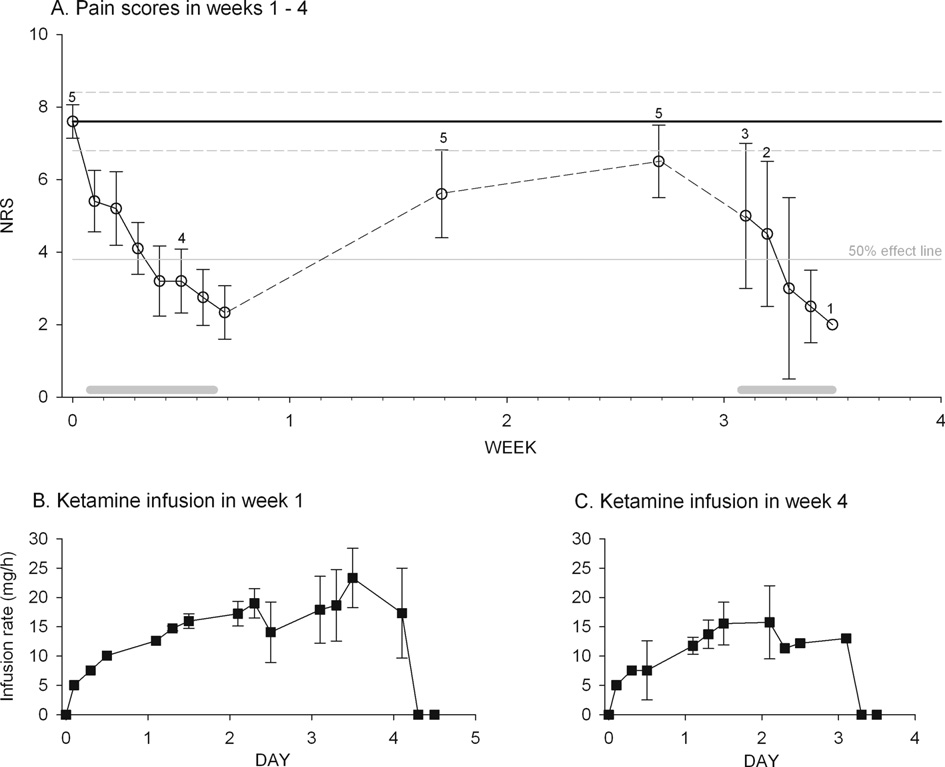
The course of pain relief and ketamine infusion scheme, an
pain score was reduced to 1. Side effects were again present, but
average plot of the pain scores and ketamine infusion rates is given
they seemed of lesser intensity compared to the first admission.
in for 5 patients of Group 1 (data from patient D are excluded
For nausea, domperidone was given. Routine blood screening on
in this graph). Since the study was single blind and not placebo-
day 3 revealed elevated liver enzymes ALP, ALT, AST, TBIL,
controlled, these data do not constitute efficacy data, but do give
and cGT exceeded the upper reference values). The ketamine infu-
an impression of the effect of treatment on pain scores.
sion was ended on that same day (total dose given, 800 mg). Thepatient had no fever, jaundice, abdominal tenderness, or enlarge-
ment of the liver. The following tests were performed: renal func-tion; clotting time; serum concentrations of ammonia and lactate;
Ketamine is increasingly used for the treatment of chronic pain.
serology for hepatitis A, B, and C; cytomegaly virus; Epstein-Barr
Data from recent trials suggest that prolonged or repetitive admin-
virus; and antinuclear, antimitochondrial, and antismooth muscle
istrations of this agent are needed to induce long-term pain relief,
antibodies. All tests were normal or negative except for the antinu-
that is, pain relief outlasting the treatment period for a period long-
clear antibody, which was weakly positive. An ultrasound of the
er than 48 h . In a previous study we showed that a single con-
liver, bile ducts, and related vasculature showed no abnormalities.
tinuous 100-hour infusion of ketamine produces the relief of CRPS
On day 4 the patient developed a severe itch of both feet and pete-
pain for up to 11 weeks, compared to placebo This is a some-
chiae. The CRPS seemed to flare up with edema of the right foot
what disappointing effect and prompted us to examine the effect of
and an increase in pain score to 6. The patient was discharged on
a second 100-hour infusion period on pain relief in CRPS-1 pa-
day 5, after which liver enzymes slowly decreased and the itch
tients. A pilot study was designed to explore possible time frames
and petechiae disappeared over a course of days to weeks. The liver
for ketamine re-administration (4 weeks vs 13 weeks). Apart from
enzymes normalized within 2 months.
the expected psychotropic and hypertensive side effects, weencountered a problem that so far was considered a rare side effect
3.6. Patient F: a 46-year-old man with CRPS of the left arm
of ketamine administration—elevation of serum liver enzymes—ata relatively high frequency. In 3 patients in study Group 1, the in-
Before treatment, the CRPS pain score was 8. Upon ketamine
crease in liver enzymes was detected just prior or during a second
infusion, a slow decline in pain score occurred with no side effects
ketamine administration, 16 days after an initial 100-hour
apart from mild sedation. During the course of the week, the
treatment. We relate the cause of elevated liver enzymes to
patient experienced various episodes of sub-febrile temperature
ketamine-induced hepatotoxicity in patients A and E, as there
(37.9 °C) without any signs of illness, infection, or allergy. At dis-
was an evident chronological relation between the ketamine infu-
charge, pain score was 4. Upon admission in week 4, the CRPS pain
sion and the development and resolution of the liver injury (e.g.,
score had increased to 7. The ketamine treatment was started but
liver enzymes declined rapidly upon termination of treatment).
I.M. Noppers et al. / PAINÒ 152 (2011) 2173–2178
Fig. 4. Pain data and infusion rates of 5 subjects showing an analgesic response during treatment with ketamine (given in a single-blind fashion). (A) Numerical rating scoresfrom week 1 to the end of week 4. The continuous black line is the pretreatment baseline mean numerical rating score ± 95% confidence interval (dashed gray lines); thecontinuous gray line is the 50% effect line. The numbers indicate the number of patients from which the pain data was obtained. (B) Ketamine infusion rates (mg/h) for thefirst treatment week (week 1). (C) Ketamine infusion rates for the second treatment week (week 5). Values are mean ± SEM. In graphs A and B, the baseline mean ± 95%confidence interval is shown (continuous black line ± dashed gray lines); in graph A, the 50% effect line is given (continuous gray line).
The cause of the liver enzyme elevation in patient F is less clear and
made thereafter . Sporadic reports of liver injury do appear
is possibly related to the ketamine treatment. We made the deci-
. For example, in refractory CRPS patients receiving keta-
sion to end the trial, as we argued that repetitive long-term keta-
mine in anesthetic dosages for 5 days, modest elevations in liver en-
mine infusions within a short time frame is a risk factor for liver
zymes were noted in 16 (of 20) patients on the last days of treatment
cell damage and we therefore concluded that our study design
Following treatment, the enzymes returned to reference values
(in Group 1 patients) is not acceptable. These data contrast findings
within 10 to 14 days. In another study, low-dose ketamine given to
in our previous study: Patients in the Sigtermans et al. trial
CRPS patients caused elevated liver enzymes in 4 (of 33) patients
received a single 100-hour infusion of ketamine with an average
during a first treatment period (duration of treatment ranged from
ketamine dose of 2.5 g (range 1.7–3.3 g) without any signs of liver
4 to 20 days; ketamine infusion rate 10–50 mg/h) One of these
toxicity or side effects beyond the duration of treatment. Some of
patients who required additional treatments 3 months later devel-
the patients in the current study use co-medication that may have
oped immediate elevations of his liver-enzyme profile during 2
had an effect on liver function.
more treatment attempts. More frequent incidence of liver damageis observed following frequent recreational ketamine abuse
4.1. Ketamine-induced liver injury
These patients often present with kidney injury,elevated liver enzymes, and bladder dysfunction. Some of these
The first reports on an association between ketamine and liver in-
patients have epigastric pain, but in most cases the elevated liver
jury date from 1979–1980. In the isolated rat hepatocyte, supraclin-
enzymes were discovered upon blood examination when the
ical doses of ketamine inhibited gluconeogenesis, and urea
patients came in for urinary tract symptoms .
formation from alanine caused a reduction in adenosine triphos-
All of the above studies that reported liver injury in response to
phate concentration and a dose-dependent leakage of L-lactate
ketamine treatment used a racemic ketamine mixture. In our study
dehyrogenase Dundee et al. described a higher incidence
we administered the S(+) enantiomer indicating that the enantio-
of significant elevations in liver enzyme levels in patients receiving
selective use of ketamine will not protect the patient for possible
3–4 mg/kg ketamine for induction and maintenance of general anes-
liver injury.
thesia compared to ‘‘standard'' techniques (involving halothane andthiopentone). Fourteen (of 34) patients receiving ketamine and 7 (of
4.2. Drug-induced liver injury (DILI)
34) receiving standard treatment had signs of liver injury. Moststudies on the use of ketamine for chronic pain treatment either
Drug-induced liver injury is unpredictable (ie, not dose related,
did not measure liver enzymes or found an absence of changes in
and difficult to reproduce in animal models) and is considered to
plasma liver enzymes . For example, in 30 patients receiv-
have a rare incidence . Various forms have been described
ing a 100-hour continuous infusion of ketamine (infusion rate be-
(hepatitis, cholestasis, cirrhosis, granulomas, steatosis, neoplas-
tween 10 and 20 mg/kg), no effect on liver enzymes was observed
mas, vascular). DILI may have immune-mediated (allergic) and
during the ketamine treatment period, but no measurements were
non-immune-mediated (nonallergic) features. In the allergic form,
I.M. Noppers et al. / PAINÒ 152 (2011) 2173–2178
the innate immune system responds to the drug or its metabolite
fully monitoring the myriad of short- and long-term side effects
as if it was a toxic foreign body or infectious organism causing a
linked to ketamine treatment.
sterile inflammatory response. In the nonallergic form, mitochon-drial impairment, oxidative stress, and cellular adaptation failure
Conflict of interest statement
are causative factors. Allergic DILI has a latency period of 1–6 weeks, with a high incidence of fever, rash, and eosinophilia, is
None of the authors report any competing interests relating to
not dose related, and recurs upon drug re-challenge. Nonallergic
the topic of this paper.
DILI has a latency of 1 month to 1 year and is possibly dose related,while the occurrence of rash, fever, and eosinophilia is uncommon.
On the basis of the liver enzyme level, DILI is classified into hep-
atitis, cholestatis, or a mixed pattern . DILI is defined as hepa-
This study was funded in part by the TREND (Trauma RElated
titis when ALT P 3�ULN (where ULN = upper limit of the normal
Neuronal Dysfunction) organization (Delft, The Netherlands), a
(ALT/ULN)/(ALP/ULN) P 5;
non-profit consortium of academic hospitals, technical research
ALP P 2�ULN and (ALT/ULN)/(ALP/ULN) 6 2; and mixed when
groups, and companies focused on the study of Complex Regional
2 < (ALT/ULN)/(ALP/ULN) < 5. In severe cases of DILI, the patient
Pain Syndrome type 1.
may develop acute liver failure defined by coagulopathy (interna-tional normalized ratio P 1.5) and hepatic encephalopathy occur-
ring in the 6 months following the onset of DILI. On the basis ofthese definitions, the clinical features, and additional laboratory
[1] Amr YM. Multi-day low-dose ketamine infusion as adjuvant to oral gabapentin
tests, we diagnosed patients A and E as having ketamine-induced
in spinal cord injury related chronic pain: a prospective, randomized, doubleblind trial. Pain Physician 2010;13:245–9.
hepatitis of the allergic form. While the cause of elevated enzymes
[2] Bell RF, Moore RA. Intravenous ketamine for CRPS: making too much of too
in patient F is likely to be the administration of ketamine in week 1,
little? Pain 2010;150:10–1.
the nature of the hepatotoxicity remains unknown. For patients A
[3] Blunnie WP, Zacharias M, Dundee JW, Doggart JR, Moore J, McIlroy PDA. Liver
and E, it remains unclear whether co-medication played an addi-
tional role in the development of DILI. For example, patient A used
[4] Bruehl S, Harden RN, Galer BS, Saltz S, Bertram M, Backonja M, Gayles R, Rudin
paracetamol (acetaminophen). While this drug is associated with
N, Bhugra MK, Stanton-Hicks M. External validation of IASP diagnostic criteriafor Complex Regional Pain Syndrome and proposed research diagnostic
nonallergic DILI, it may have enhanced ketamine-induced liver in-
criteria. International Association for the Study of Pain. Pain 1999;81:147–54.
jury. In a rat study, a synergistic hepatotoxic effect (increases in
[5] Chan WH, Sun WZ, Ueng TH. Induction of rate hepatotoxic cytochrome P-450
ALT and AST) was observed for ketamine and the solvent carbon
by ketamine and its toxicological implications. J Toxicol Environ Health A2005;68:1581–97.
tetrachloride A similar mechanism may possibly occur for par-
[6] Childers Jr WE, Baudy RB. N-methyl-D-aspartate antagonists and neuropathic
acetamol and ketamine. Further studies are needed to study para-
pain: the search for relief. J Med Chem 2007;50:2557–62.
cetamol ketamine interaction on liver function. Also, contraceptive
[7] Chizh BA. Low dose ketamine: a therapeutic and research tool to explore N-
pills are associated with elevated liver enzymes. Only patient C
methyl-D-aspartate (NMDA) receptor-mediated plasticity in pain pathways. JPsychopharmacol 2007;21:259–71.
used these, without liver enzyme elevations during the ketamine
[8] Chu PSK, Kwok SC, Lam KM, Chu TY, Chan SWH, Man CW, Ma WK, Chui KL, Yu
MK, Chan YC, Tse ML, Lau FL. ‘Street ketamine'-associated bladder dysfunction:
Warning signs for the development of DILI include abdominal
a report of ten cases. Hong Kong Med J 2007;13:311–3.
[9] Correll GE, Maleki J, Gracely EJ, Muir JJ, Harbut RE. Subanesthetic ketamine
pain, nausea/vomiting, and jaundice . However, during keta-
infusion therapy: a retrospective analysis of a novel therapeutic approach to
mine treatment, nausea and vomiting may occur from ketamine it-
complex regional pain syndrome. Pain Med 2004;5:263–5.
self, and abdominal pain may be absent due to analgesia. We
[10] Cyrek P. Side effects of ketamine in the long-term treatment of neuropathic
pain. Pain Med 2008;9:253–7.
therefore advise frequent testing during long-term ketamine treat-
[11] Dundee JW, Fee JPH, Moore J, McIlroy PDA, Wilson DB. Changes in serum
ment, especially when repeated ketamine infusions are given with-
enzyme levels following ketamine infusions. Anaesthesia 1980;35:12–6.
in short time frames. Treatment of ketamine-induced DILI is by
[12] Kalia LV, Kalia SK, Salter MW. NMDA receptor in clinical neurology: excitatory
times ahead. Lancet Neurol 2008;7:742–55.
prompt discontinuation of the exposure to ketamine and support-
[13] Kato Y, Homma I, Ichiyanagi K. Postherpetic neuralgia. Clin J Pain
ive/symptomatic treatment. In severe allergic hepatitis with no
improvement upon drug removal, a 1-week treatment with ste-
[14] Kiefer RT, Rohr P, Ploppa A, Dieterich HJ, Grothusen J, Koffler S, Altemeyer KH,
Unertl K, Schwartzman RJ. Efficacy of ketamine in anesthetic dosage for the
roids may be attempted, although proof for efficacy is limited at
treatment of refractory complex regional pain syndrome: an open-label phase
II study. Pain Med 2008;9:1173–201.
In summary, a study designed to explore the effect of repeated
[15] Nathwani RA, Kaplowitz N. Drug hepatoxicity. Clin Liv Dis 2006;10:207–17.
100-hour ketamine infusions on pain relief in CRPS patients was
[16] Ng SH, Tse ML, Ng HW, Lau FT. Emergency department presentation of
ketamine abusers in Hong Kong: a review of 233 cases. Hong Kong Med J
ended prematurely due to the development of ketamine-induced
hepatitis of allergic nature in 2 patients. In a third patient, liver in-
[17] Noppers I, Niesters M, Aarts L, Smith T, Sarton E, Dahan A. Ketamine for
jury was observed, although its origin cannot be confirmed with
certainty. All affected patients (n = 3) received 2 ketamine expo-
[18] Poon TL, Wong KF, Chan MY, Fung KW, Chu SK, Man CW, Yiu MK, Leung SK.
sures within 4 weeks' time, while patients receiving ketamine at
Upper gastrointestinal problems in inhalational ketamine abusers. J Dig Dis
a wider time interval (12 weeks, n = 3) had no signs of liver injury.
[19] Sear JW, McGivan JD. Cytotoxicity of i.v. anaesthetic agents on the isolated rat
Liver enzyme levels returned to normal in all patients within
hepatocyte. Br J Anaesth 1979;51:733–9.
2 months following the discontinuation of treatment. Patients that
[20] Selby NM, Anderson J, Bungay P, Chesterton LJ, Kohle NV. Obstructive
receive long-term or repetitive ketamine infusions for the treat-
nephropathy and kidney injury associated with ketamine abuse. NDT Plus2008;5:310–2.
ment of chronic pain should receive regular monitoring of blood
[21] Sigtermans M, van Hilten JJ, Bauer MCR, Arbous MS, Marinus J, Sarton EY,
pressure and psychotropic side effects. Furthermore, as suggested
Dahan A. Ketamine produces effective and long-term pain relief in patients
by our current report of 3 cases, regular measurements of liver
with complex regional pain syndrome type 1. Pain 2009;145:304–11.
[22] Verma S, Kaplowitz N. Diagnosis, management and prevention of drug-
function are strongly advisable. Whether ketamine treatment
induced liver injury. Gut 2009;58:1555–64.
should be extended to chronic pain patients other than CRPS type
[23] Wong SW, Lee KF, Wong J, Ng WWC, Cheung YS, Lai PBS. Dilated common bile
1 requires further study, with the need for high-quality random-
ducts mimicking choledochal cysts in ketamine abusers. Hong Kong Med J
ized trials, not only focusing on analgesic efficacy, but also care-
Source: http://www.shade.id.au/GATE%20ketamine%20and%20LFT%201%20.pdf
Etwa 32 Mil ionen Deutsche leiden unter einer Venenschwäche. Krampfadern (Vari-zen) sind die am häufigsten vorkommende Beschwerdeart: Bei ungefähr der Hälfte al er Mitteleuropäer im Alter zwischen 25 und 74 Jahren treten sie insbesondere an den Beinen auf. Meist erschlaffen hierbei die Venenwände in Folge einer Bindege-websschwäche, die Venenklappen können nicht dicht schließen und das Blut fließt als Folge nicht mehr ausreichend ab. Stattdessen staut es sich in den oberflächlichen Venen an, welche sich durch die dauerhafte Erweiterung deutlich sichtbar bläulich bis lila unter der Haut entlang schlängeln. Im Gegensatz zu Besenreisern – kleinsten erweiterten Venen, die ähnlich der Form eines Reisigbesens durch die Haut schimmern (lesen Sie hierzu auch unseren Patientenratgeber zum Thema) – stel en Krampfadern nicht nur ein ästhetisches Problem dar, sondern können auch gesundheitliche Beschwerden wie etwa geschwollene Füße und schwere, schmerzende Beine verursachen. Es ist daher sinnvol , bei entsprechend auftretenden Symptomen möglichst frühzei-tig medizinischen Rat einzuholen. Schwerwiegenderen Komplikationen wie dem Entstehen von Venen-entzündungen, Geschwüren oder Blutgerinnseln kann so vorgebeugt werden.
BMJ 2015;350:h231 doi: 10.1136/bmj.h231 (Published 11 February 2015) Sugar: spinning a web of influence Public health scientists are involved with the food companies being blamed for the obesity crisis,reports Jonathan Gornall Jonathan Gornall freelance journalist, Suffolk, UK An investigation by The BMJ has uncovered evidence of the