Levitra enthält Vardenafil, das eine kürzere Wirkdauer als Tadalafil hat, dafür aber schnell einsetzt. Männer, die diskret bestellen möchten, suchen häufig nach levitra kaufen ohne rezept. Dabei spielt die rechtliche Lage in der Schweiz eine wichtige Rolle.
Acne inversa
Review Article 189
Acne inversa
Daniela Meixner, Sylke Schneider, Markus Krause, Wolfram SterryDepartment of Dermatology, Venereology and Allergy, Charité, Berlin, Germany
JDDG; 2008 • 6:189–196
Submitted: 11.10.2006 Accepted: 30.5.2007
Acne inversa is a chronic inflammatory skin disease featuring cutaneous and
• hidradenitis suppurativa
subcutaneous nodular inflammation, fistula formation and discharge of foul-
• apocrine acne
smelling secretions.The disease can lead to functional impairment and psycho-
• pyodermia fistulans sinifica
logical problems.There is inflammation of the terminal hair follicles in intertrig-
• follicular retention tetrad
inous regions, especially perianal, axillary and inguinal areas. Less often there issubmammary, periumbilical, retroauricular or nuchal involvement.
Without treatment the disease is chronic and progressive. The causes of acneinversa are multifactorial and pathogenesis is still not well understood. Besidesa positive family history, obesity and cigarette smoking are trigger factors. Earlydiagnosis and therapy of acne inversa saves the patient years of suffering.
The most effective treatment is undoubtedly the radical wide excision of theaffected areas. Local measures such as radiotherapy, photodynamic therapyand cryotherapy have provided little benefit; the same is true for systemicantibiotic treatment or hormonal therapy with anti-androgens. TNF-alphaantagonists seem to have a promising influence on the disease. Further studiesinvestigating the effect of these substances on acne inversa are warranted.
1 Historical background
with acne conglobata and perifolliculitis
neous nodular inflammation, fistulas
The Paris surgeon Velpeau described an
capitis abscendens et suffodiens (dissect-
and discharge of a foul-smelling secre-
unusual inflammatory process with for-
ing cellulitis of the scalp) as acne triad.
tion and capable of causing severe phys-
mation of superficial axillary, submam-
For the first time, it was discussed that
ical and mental impairment.
mary and perianal abscesses in 1839 [1].
the pathogenetic mechanism of acne
Pathogenetically, it is an inflammation
His colleague Verneuil, also working in
vulgaris and acne inversa are similar.
of terminal hair follicles manifesting in
Paris, coined the term "hidrosadénite
Plewig and Kligman added another enti-
intertriginous skin at perianal, inguinal
phlegmoneuse" 15 years later [2]. This
ty to acne triad, pilonidal sinus [5]. In
and axillary sites. In addition to familial
name reflects the former pathogenetic
1989 Plewig and Steger introduced the
occurrence, smoking and obesity are
model of acne inversa, which considered
term acne inversa which is in use today,
contributing factors to the disease.
inflammation of sweat glands as the
indicating a follicular source of the dis-
Treatment of choice is the radical exci-
cause of the disease. This concept was
ease [6] and replacing older terms such
sion of affected regions.
followed by a variety of authors for many
as Verneuil disease, hidradenitis suppu-
decades. In 1922 Schiefferdecker suspected
rativa, apocrine acne and pyoderma fis-
a pathogenic association between acne
tulans sinifica (Table 1).
The exact prevalence of acne inversa is
inversa and apocrine sweat glands [3].
unknown and has been estimated at
In 1956 Pillsbury et al. [4] postulated
2 Definition
0.3 % [7]. Jemec et al. [8] report a point
follicular occlusion as cause of acne
Acne inversa is a chronic inflammatory
prevalence of 4.1 % in a collective of
inversa, which they grouped together
skin disease with cutaneous and subcuta-
young adults. The average age of these
The Authors • Journal compilation Blackwell Verlag, Berlin • JDDG • 1610-0379/2008/0603-0189
JDDG 3˙2008 (Band 6)
The course of the disease, onset only after
Table 1: Historical view.
puberty, improvement after menopauseand during pregnancy all suggest an
influence of sexual hormones. Most
First description of the disease
patients with acne inversa have normalandrogen levels [9]. Case reports do exist
of successful therapy with anti-andro-
Acne triad (hidradenitis suppurativa,
perifolliculitis capitis abscendens et suffodiens)
4.2.2 Genetic factors
Plewig/Kligman [5]
Acne tetrad (acne triad + pilonidal sinus)
Acne inversa often occurs in a familial
Plewig/Steger [6]
fashion, so that genetic factors probablyplay a role. The first study on a possiblehereditary pattern was performed by
patients was 42 years for men and smoking has a positive effect on the
Fitzsimmons et al. in 1984. Three fami-
39 years for women.
course of the disease but prospective
lies with 21 family members affected by
In a study from 1996 Jemec found a
studies are lacking. Obesity is probably
acne inversa were examined. In one of
clear predominance of women. He stud-
not directly involved in the development
the three families studied, family mem-
ied the incidence of acne inversa in a col-
of acne inversa, but maceration and
bers in three generations were affected,
lective of 507 patients. Anogenital
occlusion in the body folds lead to follic-
in the other two families; two genera-
lesions are significantly more frequent in
ular hyperkeratosis and thus worsen the
tions each with acne inversa were report-
women than in men (odds ratio 4.6),
while axillary lesions were equally dis-
In 45 % of patients with acne inversa
One year later the authors expanded
tributed among the genders [8]. Further,
sweating and heat; in 35 %, stress and
their study and examined 26 patients
Jemec et al. studied the prevalence of
exhaustion; and in 16 %, wearing tight
with acne inversa and their families.
acne inversa in an unselected collective
clothing leads to deterioration of the dis-
Information on family history could be
of 793 randomly selected individuals; 3
ease [14]. A variety of factors is blamed
obtained from 23 patients. Among 14
women and 3 men with acne inversa
with a causal relationship in the patho-
patients a total of 37 further affected
were found [5]. A higher proportion of
genesis of acne inversa. Included is use of
family members were found. In nine
women was confirmed by Barth et al. He
deodorants and depilatory products or
families the patients were the only clear-
observed 10 men and 36 women who
shaving of the involved sites. In a retro-
ly affected family member [7].
were admitted as inpatients for surgical
spective study done by Morgan et al.
In 2000 the working group of Werth et
treatment of acne inversa [9].
comparing 40 patients with acne inversa
al. studied the reproducibility of the
The disease is quite rare before puberty
with 40 healthy subjects, no significant
autosomal dominant inheritance postu-
[10]. In the fifth decade of life, the inci-
difference regarding the factors men-
lated by Fitzsimmons et al. using the
dence decreases. In women, the disease
tioned above could be found [15]. We
same study group as then. Here, 14 sur-
can continue into menopause, new man-
assume that these factors at most play a
viving persons and their families were
ifestations after menopause are rarities.
secondary role in the development and
examined. Of these, 7 had stated a posi-
aggravation of acne inversa.
tive family history in the previous study,
two, on the other hand, had stated a
4.1 Exogenic factors
4.2 Endogenous factors
negative or only possible family history.
The exact etiology of acne inversa is not
4.2.1 Hormonal factors
In the patient collective with a positive
known. Smoking is without doubt asso-
Essential for the pathogenesis of acne
family history, 27 % of first-degree rela-
ciated with the development of acne
inversa is the effect of androgens in the
tives were affected by the disease.
inversa. A series of studies has confirmed
formation of terminal heir follicles in the
Additionally, seven newly affected per-
a significantly larger proportion of
axillae and anogenital regions, as acne
sons, who were not yet affected in the
smokers in patient collectives with acne
inversa is primarily an inflammatory dis-
previous study, were found. An analysis
inversa in comparison to control groups.
ease of terminal heir follicles and not, as
of the pedigrees [17] shows that the dis-
The proportion of patients with acne
presumed in the past, a disease of apoc-
ease is transmitted through several gener-
inversa who smoke regularly is reported
rine glands. This is also exemplified by
ations of a family with acne inversa and
at 84–89 % compared to the proportion
the fact that terminal hair follicles on the
affects both genders.
in control groups between 23–46 %
scalp are not connected with apocrine
[11]. The pathogenetic mechanism by
glands, but clinical manifestations such
4.3 Microbiologic data
which smoking leads to acne inversa is
as perifolliculitis capitis abscedens et suf-
The role of bacterial colonization and/or
unknown. Smoking induces chemotaxis
fodiens (dissecting cellulitis of the scalp)
infection in the pathogenesis of acne
in neutrophilic granulocytes. This mech-
do occur. This no longer can develop in
inversa is discussed controversially. For a
anism possibly plays a role in the etiolo-
the face of androgenetic alopecia. With
long time it was presumed that contami-
gy of palmoplantar pustulosis [12] and
the onset of puberty, the secretion of
nation or infection by specific microor-
may be involved in the development of
androgens begins and thus the enlarge-
ganisms belong to the triggering factors
acne inversa. We presume that stopping
ment of hair follicles.
of the disease [19]. Lapins et al. described
JDDG 3˙2008 (Band 6)


the presence of Staphylococcus aureus and
seen. Pressure can cause secretion of pus,
development of squamous cell carcino-
coagulase-negative streptococci [20]. In
sebum or a foul-smelling secretion. At a
ma on the basis of chronic inflamma-
a retrospective review of data, Brook and
later point in time the disease is charac-
tion. A series of case reports exists in the
Frazer studied the microbiologic spec-
terized by numerous scarred areas as the
literature, but they do not allow for an
trum of 17 samples from axillary lesions
result of burned out inflammatory
estimation of the incidence of malignant
of patients with acne inversa. A total lesions (Figure 2).
tumors in acne inversa. Usually long-
of 42 cultures were performed. The
term presence of acne inversa for about
most common aerobic organisms were
5.2 Clinical spectrum
20 years is a prerequisite for the develop-
Staphylococcus aureus, Streptococcus pyo-
Clinical forms of manifestation of acne
ment of squamous cell carcinoma [24].
genes and Pseudomonas aeruginosa. The
inversa are diverse. In addition to typical
Men are predominantly affected.
most common anaerobes found were
clinical presentations in the above-men-
peptostreptococci, Prevotella and
tioned sites of predilection, acne
5.3.4 Chronic lymphedema
fusobacteria [21]. Highet et al. found
keloidalis nuchae, folliculitis abscedens
In the course of the disease recurrent
Streptococcus milleri in three cases of severe
et suffodiens (dissecting cellulitis of the
infections, for example with streptococ-
acne inversa in the anogenital region.
scalp) as well as the rarely observed cutis
ci, as well as the formation of elephanti-
This is a bacterium often found in the
vertices gyrate-like acne inversa belong
asis-like swellings mainly in the genital
gastrointestinal tract and the female gen-
to the broad spectrum of clinical presen-
region can occur [25].
ital tract and is presumed to correlate
tations. The latter is a form of scalp
with disease activity of acne inversa [19].
involvement with folds resembling sulci
5.3.5 Anemia
It is unclear at present if bacterial colo-
and gyri of the brain, sinus tracks and
Due to chronic inflammation anemia
nization and infection are primarily or
discharge of secretion [22].
has been reported in patients with acne
secondarily included in the developmen-
inversa [26].
tal process of acne inversa. Obviously, a
5.3 Complications
very heterogenous spectrum of pathogens
5.3.1 Reduced mobility
5.4 Disease burden
exists, so that the development of advanced
Healing of areas affected by acne inversa
Subjectively patients complain about
stages of the disease is not bound to the
with scarring can lead to contractures
limited mobility and pain. In severe
presence of a specific pathogen.
and greatly limit the mobility of the
cases the patients are in reduced general
limbs. This is especially true for axillary
health. Due to feelings of shame, the dis-
5 Clinical features
manifestations of the disease.
ease causes a great mental burden result-
5.1 Course
ing in social withdrawal. In a study by
Clinical manifestations in early stages of
5.3.2 Fistulas
Werth a distinctly reduced quality of life
the disease include giant comedones and
Anogenital disease is frequently accompa-
in patients with acne inversa was meas-
firm palpable nodules. In the further
nied by anal, rectal or urethral fistulas [23].
ured using the Dermatology Life
course these can coalesce deeply and
Quality Index (DLQI). A total of 114
form large abscesses and sinus tracts 5.3.3 Development of malignant tumors
patients, 16 men and 98 women, were
(Figure 1). Additionally, darkly colored,
The most severe complication of acne
examined. The DLQI score correlated
infiltrated inflammatory plaques are
inversa of the anogenital region is the
significantly with the number of inflam-matory lesions. In comparison topatients affected by other skin diseases,the quality of life of patients with acneinversa was lowest with an averageDLQI score of 8.9 [14].
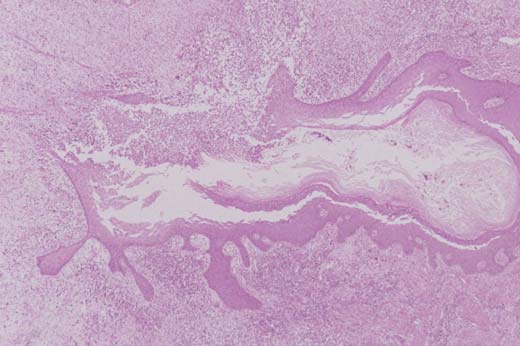
6 Histology
Published studies on histopathologic
changes have contributed greatly to
understanding the disease acne inversa.
Plewig and Steger view the hyperkerato-
sis of the follicular infundibulum with
subsequent bacterial superinfection and
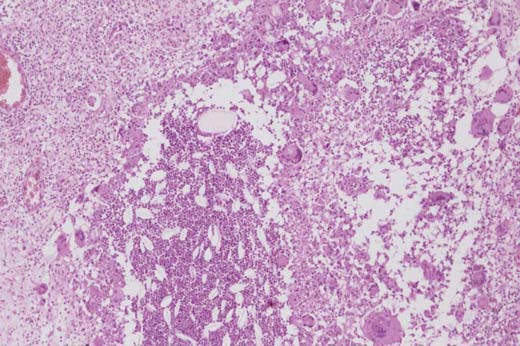
rupture of the follicle (Figure 3) and the
resulting inflammation of connective tis-
sue (Figure 4) as primary events.
Histologically, the apocrine and eccrine
sweat glands are not involved primarily,
but secondarily [6]. Yu et al. examined
12 histological samples of patients with
acne inversa and found cysts and sinus
tracts lined by epithelium in the dermis
Figure 1: Axillary lesions of acne inversa with sinus
Figure 2: Axillary lesions of acne inversa with dermal
in 10. About one-half of the sinus tracts
JDDG 3˙2008 (Band 6)
contained free hair shafts. In about one-third of the samples inflammation of theapocrine sweat glands with simultaneousinflammation of the eccrine sweat glandsand hair follicles was found [27]. In astudy by Jemec et al. the majority ofsamples (44 of 51) revealed occlusion ofthe tracts and cysts and follicles. Primaryinflammation of apocrine glands was notseen [28]. Boer and Weltervreden werealso able to demonstrate a primaryinflammation of the follicular infundibu-lum and secondary involvement of apoc-rine sweat glands (Table 2) [29]. On the other hand, inflammation of thehair follicle without involvement of theassociated apocrine sweat glands is oftenseen [6]. The inflammatory reaction is
Figure 3: Rupture of hair follicle with inflammatory cell infiltrate.
quite mixed consisting of an unspecificlymphohistiocytic infiltrate, plasma cells,mononuclear cells and neutrophilicgranulocytes. Histological features are quite unequivo-cal and allow making differential diag-noses which are clinically difficult andrule out entities such as furunculosis,irritated sebaceous gland retention cysts,perianal Crohn disease or multiple sweatgland abscesses.
7 Differential diagnoses/associated
diseases
In initial stages of acne inversa differen-
tial diagnosis includes furuncles and car-
buncles caused by staphylococci and
streptococci. At the initial visit other
pathogen-induced diseases such as deep
fungal infections, actinomycosis and
Figure 4: Granulomatous inflammation with foreign body giant cells.
sporotrichosis should be excluded. In thegroin or anogenital region, lymphogran-
Table 2: Dermatohistological view.
uloma venereum and granulomainguinale are additional considerations.
Further differential diagnoses are granu-
Initial hyperkeratosis of the follicular
lomatous diseases such as tuberculosis
cutis colliquativa or cutaneous fistulas in
Bacterial superinfection and follicle rupture
Crohn disease (Table 3).
Plewig et al. [6]
Granulomatous inflammatory reaction of the
Clinical differentiation from Crohn dis-
connective tissue
ease can be particularly difficult, as in
Apocrine and eccrine sweat glands secondarily
5 % of all cases of Crohn disease perianal
lesions are the initial manifestation [28].
In a study by Church et al. 38 % of patients
Cysts and sinus tracts lined with epithelium,
with acne inversa examined had simultane-
in part with hair shafts
ous Crohn disease (n = 61 patients). The
Inflammation of apocrine sweat glands only
diagnosis of Crohn disease preceded acne
if eccrine sweat glands and hair follicles are
inverse by 3.5 years on average [30].
Primary inflammation of the follicular
8 Treatment
8.1 Surgical treatment
Apocrine sweat glands secondarily involved
Treatment method of choice is the totalexcision of affected skin areas.
JDDG 3˙2008 (Band 6)
the extent of surgery [32]. This was con-
Table 3: Differentiation points.
firmed in a study by Ritz et al. Here, thelong-term results of three differing surgi-
Differential diagnoses
cal procedures were followed over up to72 months postoperatively. The compar-
Follicular nodule,
Bacteriologic identifi-
ison revealed a recurrence rate of 100 %
rapid enlargement,
cation of Staphylococ-
in patients treated with incision and
fluctuation and possi-
drainage, a recurrence rate of 42.8 % in
Diagnosis is made
patients treated with narrow excision of
the lesions as well as a recurrence rate of27 % in patients with wide excision of
Inflammatory lesions
Identification with
lesions in healthy tissue [33].
Deep fungal infection
direct microscopy and
For axillary lesions postoperative diffi-
follicular abscesses
culties are slight, but the recurrence rate
Histologic identifica-
is higher for primary wound closure than
mandibular region,
for secondary intention healing [34].
Gram stain, anaerobic
Varying statements on the extent of exci-
sion, which correlates with recurrencerates, exist. The tissue block to be excised
Histologic identifica-
should include not only lateral but also
tion of cigar-like yeast
deep safety margins.
Often subcutaneous
cells in the PAS stain,
Although the healing process is more
nodes occurring on the
Culture at 37 °C (yeast
rapid with a split-thickness graft, patients
arms, spread along
colonies) and at 25 °C
usually prefer healing by secondary
lymphatic vasculature
(colonies of hyphal
intention. Advantages of secondary
intention healing are a shorter hospitalstay, more rapid return to work as well asless limitation of mobility immediately
Occurrence in endemic
after surgery [35].
Initially, primary
regions (East Africa,
In our clinic radical excision of affected
papule, after 2–3
areas with secondary conditioning of the
weeks lymph node
Direct identification
wound or split-thickness grafting after
with FITC labeled
adequate granulation to prevent scar
strictures with the resulting limitation of
Livid rope-like adherent
antibodies, PCR, cul-
mobility are standard (Figures 5–9). In
swelling in the groin
ture on McCoy cell
patients with mild acne inversa who
line (inclusion bodies)
have only few inflammatory nodules andfistulas in a small area, we perform exci-
Direct identification of
sion and primary wound closure with
Papules in the genital
pathogen in a tissue
adapting sutures. We do not perform
biopsy, Giemsa stain
Granuloma inguinale
surgery on more than two extensively
affected sites in one session. Antibiotic
Culture on McCoy
therapy is administered only in case of
postoperative bacterial wound infection
Diascopy: "apple jelly"-
or preoperatively only in particularly
Often clavicular,
colored infiltrate;
severe and active acne inversa.
Tuberculosis cutis
submandibular and
cervical location
8.2 Conservative treatment
Clinical features similar
Treatment of choice for acne inversa is
Cutaneous manifesta-
Often perianal or
to acne inversa, no
without doubt the surgical procedure
tions of Crohn disease
periorificial location
described above. Due to the extent ofthis procedure and the incurrent signifi-cant surgical trauma, there has been a
Unfortunately only few studies on surgical
submammary 50 % [31]. Here, pseudo-
continual search for conservative treat-
results and recurrence rates of acne inversa
recurrences must be differentiated from
after surgical treatment exist. The largest
true recurrences. The former is the new
A small study on cryotherapy exists.
study which we are aware of reports the
manifestation of acne inversa in an untreat-
Here, marked improvement could be
following recurrence rates 3–72 months
ed hairy border area of the surgical field.
realized in 8 of 10 patients. In addition
after radical surgical excision: axillary 3 %,
It was shown that the recurrence rate
to considerable pain, in almost each case
perianal 0 %, inguinal and perineal 37 %,
after surgery correlated primarily with
complications such as infection and/or
JDDG 3˙2008 (Band 6)




Figure 7: Axillary nodular inflammation of acne inversa preoperative.
Figure 5: Axillary lesions of acne inversa before surgi-
cal excision.
Figure 8: Axillary lesions of acne inversa during operation.
Figure 6: Axillary lesions of acne inversa after skin graft.
ulceration were observed. No data onrecurrence rates were provided [36].
On the basis of knowledge on inductionof acne inversa by androgens [37], sub-stances with antiandrogenic propertieswere therapeutically tried. In a double-blind randomized study published in1986 treatment with ethinyl estradiol/cyproterone acetate and ethinyl estradi-ol/ norgestrel showed improvement in18 of 24 women treated over a follow-upperiod of 18 months [16].
The administration of 5-␣–reductasetype II inhibitors for therapy of benign
Figure 9: Axillary lesions of acne inversa after primary wound closure and insertion of an elasic strap.
JDDG 3˙2008 (Band 6)
prostate hyperplasia as well as male
study (follow-up 4–6 months) on
androgenetic alopecia suggested use for
isotretinoin, these positive effects could
Velpeau A. Aissele. In: Bechet Jeune Z:
acne inversa as well. In an open trial at a
not on the whole be documented [46].
Dictionnaire de medecine, on Reper-
dose of 5 mg daily a positive effect was
Great hope in the development of con-
toire Générale des Sciences Medicals
observed in six of seven patients treated
servative treatment modalities have been
sous le Rapport Theorique et Pratique.
(follow-up 8–24 months) [38].
raised by the introduction of TNF␣
The important role of bacterial contami-
antagonists. TNF␣ as a proinflammato-
Verneuil AS. Etudes sur les tumeurs de
nation and infection especially for signs
ry cytokine plays a key role in the devel-
la peau et quelques maladies de glandes
and symptoms of the disease such as odor,
opment of severe, chronic inflammatory
sudoripares. Arch Gen Med 1854; 94:
inflammation and suppuration particular-
reactions. Based on positive results in
ly in advanced stages of the disease sug-
treating Crohn disease with infliximab,
Schiefferdecker B. Die Hautdrüsen der
gests primary or additional antibiotic ther-
the first case report of successful admin-
Menschen und der Säugetiere, ihre hi-
apy. A retrospective evaluation of 14
istration of this monoclonal chimeric
stologische und rassenanatomische Be-
patients with long-term antibiotic therapy
IgG TNF␣ antibody for acne inversa
deutung sowie die muscularis sexualis.
is representative. Clindamycin (2 x 300 mg
was published in 2003 [ 47, 48]. An
In: Schweizerbart E (Hrsg), Stuttgart:
daily) and rifampicin (2 x 300 mg daily)
excellent response was achieved with
were administered for a 10 week period.
doses of 5 mg/kg body weight adminis-
Pillsbury DM, Shelley WB, Kligmann
In 10 patients complete healing occurred
tered as a short infusion with up to 3
AM. Bacterial infections of the skin. In:
[39]. Case reports on the administration
repetitions (week 0, 2, 6). In the first
Pillsbury DM: Dermatoloy. 1st edn.
of cyclosporine exist. In all cases improve-
case control study on this therapy, also
Philadelphia: 1956: 482–9.
ment of the condition at doses between 2
published in 2003, Sullivan et al. report
Plewig G, Kligman A. Acne. Morpho-
and 6 mg/kg body weight daily could be
an excellent response to treatment in all
genesis and Treatment. Berlin: Sprin-
observed. Due to the spectrum of side
five patients treated. Significant
ger, 1975: 192–3.
effects of cyclosporine, it does not appear
improvement was already seen after one
Plewig G, Steger M. Acne inversa (alias
suitable for the necessary long-term treat-
or two therapy cycles, while it must be
acne triad, acne tetrad or hidradenitis
ment required [40].
taken into consideration that in some
suppurativa). In: Marks R, Plewig G:
Due to clinical, histologic and patho-
cases parallel treatment with other anti-
Acne and related disorders. London:
genetic similarities between acne inversa
inflammatory agents such as pred-
Martin Dunitz; 1989: 345–57.
and Crohn disease, it has been attempt-
nisolone and cyclosporine were being
Fitzsimmons JS, Guilbert PR, Fitzsim-
ed to administer pharmacological agents
administered [49]. Cusack and Buckley
mons EM. Evidence of genetic factors
proven efficacious for Crohn disease for
reported in a first case series on 6
in hidradenitis suppurativa. Br J Der-
acne inversa, too. Methotrexate therapy
patients treated with etanercept, a fusion
matol 1985; 113: 1–8.
of three patients did not lead to the
protein with soluble TNF receptor func-
Jemec GB, Heidenheim M, Nielsen
desired effects [41].
tion. An initial response to treatment
NH. The prevalence of hidradenitis
In 2001 an open study on therapy with
was observed after (on average) 16 days
suppurativa and its potential precursor
dapsone was published. Due to positive
at a dose of 25 mg 2x weekly. About 2–3
lesions. J Am Acad Dermatol 1996; 35:
treatment results in acne conglobata,
weeks after the end of treatment, recur-
effects in acne inversa could also be
rence occurred [50]. The administration
Barth JH, Layton AM, Cunliffe WJ.
expected. A good response to treatment
of TNF␣ receptor antagonists in patients
Endocrine factors in pre- and postme-
could be documented in all five patients
with acne inversa is an off-label use.
nopausal women with hidradenitis
treated [42], but this treatment could
In summary, available data on conserva-
suppurativa. Br J Dermatol 1996; 134:
not prevail in clinical routine.
tive treatment of acne inversa does reveal
Based on the known efficacy of retinoids
some innovative approaches, that might
10 Mengesha YM, Holcombe TC, Hansen
in other forms of acne and other skin
possibly avoid surgery or perhaps can be
RC. Prepubertal hidradenitis suppurativa:
diseases accompanied by hyperkeratosis
performed preoperatively resulting in less
two case reports and review of the litera-
[43] several publications on treatment
extensive or less complicated surgery. <<<
ture. Pediatr Dermatol 1999; 16: 292–6.
with isotretinoin as well as acitretin have
11 König A, Lehmann C, Rompel R, Hap-
appeared. Due to the fact that the main
Conflict of interest
ple R. Cigarette smoking as a triggering
mechanism of action of isotretinoin is
factor of hidradenitis suppurativa. Der-
the inhibition of seborrhea, this treat-
matology 1999; 198: 261–4.
ment appears inappropriate for acne
12 O'Doherty CJ, MacIntyre C. Palmo-
inversa, as no relevant seborrhea exists
Correspondence to
plantar pustulosis and smoking. Br
here. The publications on isotretinoin
Med J 1985; 291: 861–4.
are thus controversial. A case report
Department of Dermatology,
13 Jemec GB. Body weight in hidradenitis
exists on successful treatment with
Venereology and Allergy
suppurativa. In: Marks R, Plewig G:
isotretinoin (initial dose 20 mg daily
Charité Campus Benjamin Franklin
Acne and related disorders. Martin Du-
increased to 60 mg daily), but in combi-
Fabeckstrasse 60–62
nitz, London: 1989: 375–6.
nation with prednisolone (20 mg daily)
D-14195 Berlin, Germany
14 Von der Werth JM, Jemec GB. Morbi-
[44]. An open study showed a response
Tel.: +49-30-84 45-69 01
dity in patients with hidradenitis
to therapy (follow-up 2 months) in five
Fax: +49-30-84 45-69 07
suppurativa. Br J Dermatol 2001; 144:
of eight patients [45]. In a retrospective
JDDG 3˙2008 (Band 6)
15 Morgan WP, Leicester G. The role of
26 Tennant F, Bergeron JR, Stone OJ,
38 Joseph MA, Jayaseelan E, Ganapathie
depilation and deodorants in hidra-
Mullins JF. Anemia associated with
B, Stephen J. Hidradenitis suppurativa
denitis suppurativa. Arch Dermatol
hidradenitis suppurativa. Arch Derma-
treated with finasteride. J Dermatolog
1982; 118: 101–2.
tol 1968; 98: 138–40.
Treat 2005; 16: 75–8.
16 Mortimer PS, Dawber RP, Gales MA,
27 Yu C, Cook M. Hidradenitis suppura-
39 Mendonca CO, Griffiths CEM. Clin-
Moore RA. A double-blind controlled
tiva: a disease of follicular epithelium,
damycin and Rifampicin combination
cross-over trial of cyproterone acetate in
rather than apocrine glands. Br J Der-
therapy for hidradenitis suppurativa. Br
females with hidradenitis suppurativa.
matol 1990; 122: 763–69.
J Dermatol 2006; 154: 977–8.
Br J Dermatol 1986; 115: 263–8.
28 Jemec GB, Hansen U. Histology of
40 Rose RF, Goodfield MJD, Clark SM.
17 Fitzsimmons JS, Guilbert PR. A family
Hidradenitis suppurativa. J Am Acad
Treatment of recalcitrant hidradenitis
study of hidradenitis suppurativa. J
Dermatol 1996; 34: 994–9.
suppurativa with oral ciclosporin. Clin
Med Genet 1985; 22: 367–73.
29 Boer J, Weltevreden EF. Hidradenitis
Exp Dermatol 2005; 31: 154–6.
18 Von der Werth JM, Williams HC. The
suppurativa or Acne inversa. A clinico-
41 Jemec GB. Methotrexate is of limited
natural history of hidradenitis suppura-
pathological study of early lesions. Br J
value in the treatment of hidradenitis
tiva. J Eur Acad Dermatol Venereol
Dermatol 1996; 135: 721–5.
suppurativa. Clin Exp Dermatol 2002;
2000; 14: 389–92.
30 Church JM, Fazio VW, Lavery IC,
27: 528–9.
19 Highet AS, Waren RE, Staugthon RC.
Oakley JR, Milsom JW. The differen-
42 Hofer T, Itin PH. Acne inversa: Eine
Strepococcus milleri causing treatable in-
tial diagnosis and comorbidity of hidra-
Dapson-sensitive Dermatose. Hautarzt
fection in perineal hidradenitis suppura-
denitis suppurativa and perianal Crohn's
2001; 52: 989–92.
tiva. Br J Dermatol 1980; 103: 375–82.
disease. Int J Colorectal Dis 1993; 8:
43 Akyol M, Ozcelik S. Non-acne derma-
20 Lapins J, Jarstrand C, Emtestan L. Co-
tologic indications for systemic isotreti-
agulase negative staphylococci are the
31 Harrison BJ, Mudge M, Hughes LE.
noin. Am J Clin Dermatol 2005; 6:
most common bacteria found in cultu-
Recurrence after surgical treatment of
res from the deep portions of hidra-
hidradenitis suppurativa. Br J Derma-
44 Fearfield LA, Staugthon RCD. Severe
denitis suppurativa lesions as obtained
tol 1987; 294: 487–9.
vulvar apocrine acne successfully trea-
by carbon dioxide laser surgery. Br J
32 Rompel R, Petres J. Long-term results
ted with prednisolone and isotretinoin.
Dermatol 1999; 140: 90–5.
of wide surgical excision in 106 patients
Clin Exp Dermatol 1999; 24: 189–92.
21 Brook I, Frazier EH. Aerobis and anae-
with hidradenitis suppurativa. Derma-
45 Dicken CH, Powell ST, Spear KL. Eva-
robic microbiology of axillary hidra-
tol Surg 2000; 26: 638–43.
luation of isotretinoin treatment of hid-
denitis suppurativa. J Med Microbiol
33 Ritz JP, Runkel N, Haier J, Buhr HJ.
radenitis suppurativa. J Am Acad Der-
1999; 103–5.
Extent of surgery and recurrence rate of
matol 1984; 11: 500–2.
22 Plewig G. Acne inversa, Acne keloidalis
hidradenitis suppurativa. Int J Colorec-
46 Boer J, Gemmert MJ. Long-term re-
nuchae, abszedierende Follikulitis der
tal Dis 1998; 13: 164–8.
sults of isotretinoin in the treatment of
Kopfhaut: Ein verbindendes Konzept. In:
34 Pollock WJ, Virnelli FR, Ryan RF. Axil-
68 patients with hidradenitis suppura-
Plewig G, Prinz J (Hrsg): Fortschritte der
lary hidradenitis suppurativa. A simple
tiva. J Am Acad Dermatol 1999; 40:
praktischen Dermatologie und Venerolo-
and effective surgical technique. Plast
gie. Berlin: Springer, 2002: S. 192–203.
Reconstr Surg 1972; 49: 22–7.
47 Lebewohl B, Sapadin AS. Infliximab
23 Buckley C, Sarkany I. Urethral fistula
35 Morgan WP, Harding KG, Hughes LE.
for the treatment of hidradenitis
and sinus formation in hidradenitis
A comparison of skin grafting and
suppurativa. JAAD 2003; 49: 275–6.
suppurativa. Clin Exp Dermatol 1989;
healing by granulation, following axil-
48 Rosi YL, Lowe L, Kang S. Treatment of
14: 158–60.
lary excision for hidradenitis suppura-
hidradenitis suppurativa with inflixi-
24 Perez-Diaz D, Calvo-Serrano M, Mar-
tiva. Ann R Coll Surg Engl 1983; 65:
mab in a patient with Crohn's disease. J
tinez-Hijosa E, Fuenmayor-Valera L,
Dermatol Treat 2005; 16: 58–62.
Muñoz-Jiménez F, Turéganos-Fuentes
36 Bong JL, Shalders K, Saihan E. Treat-
49 Sullivan TP, Welsh E, Kerdel FA, Bur-
F, Del Valle E. Squamous cell carci-
ment of persistent painful nodules of
dick AE, Kirsner RS. Infliximab for
noma complicating perianal hidradeni-
hidradenitis suppurativa with cryo-
hidradenitis suppurativa. Br J Derma-
tis suppurativa. Int J Colorectal Dis
therapy. Clin Exp Dermatol 2002; 28:
tol 2003; 149: 1046–9.
1995; 10: 225–8.
50 Cusack C, Buckley C. Etanercept: ef-
25 Plewig G, Kligman A. Acne and rosa-
37 Ebling FJ. Hidradenitis suppurativa: an
fective in the management of hidra-
cea. 3rd edn. Berlin: Springer, Heidel-
androgen-dependent disorder. Br J
denitis suppurativa. Br J Dermatol
berg New York: 2000: S. 309–41.
Dermatol 1986; 115: 259–62.
2006; 154: 726–9.
JDDG 3˙2008 (Band 6)
Source: http://acne-inversa-charite.de/pdf/Meixner_et_al..pdf
TRAINING ACTIVITIES FOR ACTIVIDADES DE ENTRENAMIENTO DE HABILIDADES VISO-PERCEPTIVAS Visual-Spatial Relationships (Basic Level) Relaciones Viso-espaciales (Nivel Básico) Vidal-López, Joaquín Muiños-Durán, Mónica Codina-Fossas, Marta García-Montero, María Gimeno-Galindo, Patricia TRAINING ACTIVITIES FOR ACTIVIDADES DE ENTRENAMIENTO
Issue 7 - autumn 2012 Cannon Hil Anglican Col ege magazine providing the right the chairman environment for for thought also inside:the noblest of professions the art of role model ing PSA gains momentum Pax et Bonum Issue 07 - Autumn 12