Levitra enthält Vardenafil, das eine kürzere Wirkdauer als Tadalafil hat, dafür aber schnell einsetzt. Männer, die diskret bestellen möchten, suchen häufig nach levitra kaufen ohne rezept. Dabei spielt die rechtliche Lage in der Schweiz eine wichtige Rolle.
Mmcinfo.co.za



male circumcision for Hiv prevention
WHO TecHnical advisOry GrOup On
innOvaTiOns in Male circuMcisiOn:
evaluation of
two adult devices
male circumcision for Hiv prevention
WHO TecHnical advisOry GrOup On
innOvaTiOns in Male circuMcisiOn:
evaluation of
two adult devices
WHO Library Cataloguing-in-Publication Data
Male circumcision for HIV prevention : WHO Technical Advisory Group on Innovations in Male Circumcision : evaluation of two adult devices, January 2013 : meeting report.
1.HIV infections - prevention and control. 2.Circumcision, male – therapeutic use. 3.Circumcision, male –
instrumentation. 4.Circumcision, male – methods. 5.Surgical instruments – adverse effects. 6.Risk factors.
7.Program development. 8.Guideline. 9.Adult. I.World Health Organization.
ISBN 978 92 4 150563 5
(NLM classification: WC 503.4)
World Health Organization 2013
All rights reserved. Publications of the World Health Organization are available on the WHO web site (www.who.int)
or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]).
Requests for permission to reproduce or translate WHO publications –whether for sale or for non-commercial distribution– should be addressed to WHO Press through the WHO web site (www.who.int/about/licensing/copyright_form/en/index.html).
The designations employed and the presentation of the material in this publication do not imply the expression of
any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers' products does not imply that they are endorsed or
recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in
this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
Layout by Genève Design
Printed by the WHO Document Production Services, Geneva, Switzerland
list of participants
Members
Professor Kasonde Bowa
Mr Edgar Makona
Associate Professor of Urology UNZA & CBU SOM Honorary
National Focal Point
Consultant Urologist UTH
Global Youth Coalition on HIV/AIDS
Inaugural Dean CBU School of Medicine
P.O. Box 14907, 00800, Nairobi
Head MC Unit University Teaching Hospital
UNZA School of MedicineP.O. Box 50110, Lusaka, Zambia
Dr Timothy Hallett
Ms Emily Miesse-Gumkowski
Development Engineer
Imperial College London
North Haven, CT 06473, USA
South Kensington Campus, London SW7 2AZUnited Kingdom
Dr Timothy Hargreave
Dr Pius Musau
Urological Surgeon
20 Cumin Place Edinburgh EH9 2JX
Department of Surgery
Moi University, School of MedicineNandi Road - P.O. Box 5455, 30100Eldoret, Kenya
Dr Theobald Hategekimana
Dr William Potter
Stapleford Scientific Services
University Teaching Hospital (CHU)
P.O. Box 254, Kigali, Rwanda
Professor John Krieger
Dr Christopher Samkange
Department of Urology
University of Washington
Institute of Continuing Health Education
1959 N.E. Pacific
University of Zimbabwe
Seattle, WA 98195, USA
College of Health Sciences, Harare, Zimbabwe
Dr Ira Sharlip
Dr Helen Weiss
Urological Surgeon
Chair, American Urological Association Task Force
Head of IDE and Reader in Epidemiology and
on Male Circumcision
International Health
San Francisco, CA, USA
London School of Hygiene and Tropical MedicineKeppel Street, London WC1E 7HT, United Kingdom
Dr Stephen Watya
Uro Care
P.O. Box 25974
Kampala, Uganda
Observers
Ms Melanie Bacon
Dr Emmanuel Njeuhmeli
Scientific Program Manager
Senior Biomedical Prevention Advisor
National Institutes of Health (NIH)
Global Health Bureau/Office of HIV/AIDS
9000 Rockville Pike
Technical Leadership & Research Division
Bethesda, Maryland 20892, USA
1300 Pennsylvania Avenue, MW, Washington D.C, USA
Dr Naomi Bock
Dr Jason Reed
HIV Prevention Branch, Division of Global
Senior Technical Advisor
HIV/AIDS, Centers for Global Health
Office of the US Global AIDS Coordinator
Centers for Disease Control and Prevention
2100 Pennsylvania Ave, Suite 200
1600 Clifton Rd. Atlanta, GA 30333, USA
Washington DC 20037, USA
Ms Agnes Chidanyika
Dr Renee Ridzon
Technical Specialist
United Nations Population Fund (UNFPA)
Consultant to BMGF
P.O. Box 2530, DK - 2100 Copenhagen, Denmark
Ms Celeste Sandoval
Science Advisor
UNAIDS, Geneva, Switzerland
WHO Secretariat
Dr Rachel Baggaley
Ms Julia Samuelson
Acting Coordinator
Male Circumcision Focal Point
Key Populations and Innovative Prevention
Key Populations and Innovative Prevention
Department of HIV/AIDS
Department of HIV/AIDS
Dr Gaby Vercauteren
Ms Irena Prat
Department of Essential Medicines and
Department of Essential Medicines and Pharmaceutical
Pharmaceutical Policies
Dr Buhle Ncube
Dr Emil Asamoah-Odei
Male Circumcision Focal Point
Programme Manager
HIV/Sexually Transmitted Infections
Regional Office for Africa (AFRO)
Dr Nuhu O Yaqub
Maternal, Newborn, Child Adolescent Health
Consultants
Ms Nita Bellare
Dr Doris Mugrditchian
Key Populations and Innovative Prevention
Key Populations and Innovative Prevention
Department of HIV/AIDS
Department of HIV/AIDS
Dr Timothy Farley
Dr Nicolas Magrini
Head, Drug Evaluation Unit
Nyon, Switzerland
WHO Collaborating Centre in Evidence-Based Research Synthesis and Guideline DevelopmentEmilia Romagna Health and Social Care Agency Viale Aldo Moro, 21, 40127 Bologna, Italy
acknowledgments
WHO would like to thank all the participants of the WHO
could be held in a timely manner. The principal writers of this
Technical Advisory Group on Innovations in Male Circumcision, in
report were Tim Farley, Doris Mugrditchian and Julia Samuelson.
particular, the co-chairs, Timothy Hargreave and Stephen Watya.
We also express our thanks for funding support from the Bill and
WHO would also like to acknowledge all the researchers who
Melinda Gates Foundation and the US President's Emergency
have shared data, published or confidential, so that this meeting
Plan for AIDS Relief (PEPFAR).
Department of Essential Medicines and Pharmaceutical Policies
failure modes and effects analysis
Global Harmonization Task Force
human immunodeficiency virus
Instructions for Use
International Organization for Standardization
US President's Emergency Plan for AIDS Relief
prequalification
serious adverse event
Technical Advisory Group on Innovations in Male Circumcision
Joint United Nations Programme on HIV/AIDS
Visual analogue score
Voluntary medical male circumcision
World Health Organization
executive summary
The World Health Organization (WHO) Technical Advisory
in about one year as more experience with use of the device
Group on Innovations in Male Circumcision (TAG) met at
accumulates in diverse programmatic settings outside the context
WHO headquarters in Geneva in January 2013. The focus of
the meeting was a review of the clinical performance of two specific male circumcision devices (PrePex and ShangRing) as
The PrePex (elastic collar compression) device had been
part of the product review in the WHO Prequalification of Male
evaluated in eight studies conducted in Rwanda, Uganda and
Circumcision Devices Programme. This review was based on
Zimbabwe involving about 2400 device placements. The range
clinical data collected in the context of the Framework for clinical
and scope of these studies met the criteria established in the
evaluation of male circumcision devices (WHO), which stipulates
WHO Framework for clinical evaluation of devices for male
a progressive series of clinical studies to establish the efficacy,
circumcision. About 7% of clients could not have the PrePex
safety, acceptability and clinical performance of the device when
device placed for various anatomical and technical reasons but
used by trained mid-level providers. The evaluation was also
would have been eligible for conventional surgical circumcision.
informed by the failure modes and effects analysis conducted
Circumcision was successfully completed using the PrePex in
by WHO for the collar clamp and elastic collar compression
99.5 % of clients on whom the device was successfully placed.
type devices. The meeting discussions also provided inputs on
Adverse events occurred in 1.7% of clients, the majority of
programmatic considerations for guidance under development on
which were mild or moderate. Serious adverse events occurred
the use of devices, information gaps and research needs.
in 0.4% of clients, some of whom required prompt intervention to prevent potentially serious long-term sequelae. Over half
The ShangRing (collar clamp) device had been evaluated in five
of these serious events were due to device displacement or to
studies in Kenya, Uganda and Zambia, involving almost 2000
device removal (including self-removal) secondary to pain or
device placements. These clinical studies met the minimum
discomfort. These cases resulted in pain, swelling and occasional
requirements necessary before a device can be considered for
blistering of the partially necrosed foreskin tissue, requiring
prequalification. The overall estimated proportion of clients not
urgent intervention by a skilled surgeon to prevent severe local or
eligible for male circumcision with the ShangRing device was
systemic infection and/or permanent disfigurement of the penis.
about 1%. In about one of every 200 clients, it was not possible
In the studies conducted to date, appropriate surgical facilities
to complete the circumcision procedure with the device alone.
have been available, and all cases were successfully managed
Some men required immediate conversion to conventional
with no long-term sequelae. Client instructions must clearly
surgical circumcision to avoid any serious complications. The
describe safe use of the device, symptoms that may develop with
conventional surgery was performed by a person experienced
device displacement or early removal, as well as the possible
in standard surgical circumcision who was available on site,
serious outcomes and surgical interventions that may be needed
together with appropriate instruments and supplies. The data
if instructions on abstinence and wound care are not followed.
demonstrated that the ShangRing was efficacious and safe
Similarly, PrePex providers must be appropriately trained to
when used by suitably trained and equipped providers, with a
recognize the rare serious complications that can occur if the
circumcision success rate of over 99%. No serious adverse events
device is displaced and must ensure that such clients are rapidly
occurred in 1983 successful device placements. A total of 20 men
provided appropriate management.
(1.0%) experienced moderate adverse events. All adverse events were managed with, at most, minor intervention and resolved,
On the basis of the clinical evaluation, the TAG concluded that
leaving no long-term sequelae. The adverse event rates were
the requirements for clinical studies necessary before a device is
similar to those observed with conventional surgical circumcision. considered for WHO prequalification had been satisfactorily met.
The TAG considered the device to be clinically efficacious in male
The TAG considered the ShangRing to be clinically efficacious
circumcision and safe for use among healthy men 18 years and
and safe for use in healthy men age 18 years and older, when
older when used by trained mid-level providers in public health
performed by trained providers in public health programmes.
programmes, provided that surgical backup facilities and skills
Skills and surgical facilities should always be available to safely
are available within 6–12 hours to manage events that could
convert technical failures of device placement to a conventional
lead to serious complications. The TAG based its conclusion on
procedure. The TAG based its conclusion on the data currently
the data currently available. This conclusion must be reassessed
available and recognized that this is only one component of the
in about one year as more experience and data accumulate with
prequalification assessments. This conclusion must be reassessed
use of the device in diverse programmatic settings outside the context of studies.
introduction
The HIV Department at the WHO headquarters convened
male circumcision (1), published in 2012, describes the clinical
a meeting of the WHO Technical Advisory Group (TAG) on
evaluation pathways required to provide sufficient evidence of
Innovations in Male Circumcision in Geneva, Switzerland, 29–31
efficacy and safety of a new male circumcision device. These
January 2013. The purpose of the meeting was to provide
programmatic and technical updates and to evaluate and advise on the clinical efficacy and safety of two devices for adolescent
• initial studies to establish safety and acceptability;
and adult male circumcision that have formally entered the
• at least two independent randomized control ed trials comparing
WHO prequalification process. The three-day meeting brought
the device against an established method of circumcision
together members and observers of the TAG along with the WHO
performed by providers skil ed to offer either method of male
Secretariat and staff from the HIV Department, the Department
circumcision in settings of intended final use; and
of Essential Medicines and Pharmaceutical Policies, the WHO
• at least two field studies of procedures involving relevant
Regional Office for Africa, and the Intercountry Support Team.
populations, types of facilities and performed by suitably
trained and qualified mid-level or non-physician providers in settings of intended final use.
In March 2007, responding to compelling evidence from three
The information generated from these studies forms the basis for
randomized controlled clinical trials confirming the results from
WHO to assess and provide advice on the use of a device in adult
ecological studies, WHO and the Joint United Nations Programme
and adolescent VMMC programmes for HIV prevention in high
on HIV/AIDS (UNAIDS) issued recommendations that medical
HIV prevalence, resource-limited settings.
male circumcision be considered as part of a comprehensive HIV prevention package in countries with generalized epidemics.
WHO also established the Prequalification (PQ) of Male
Since then, 14 countries in east and southern Africa have
Circumcision Devices Programme for HIV Prevention in the
taken action towards the scale-up of voluntary medical male
Department of Essential Medicines and Pharmaceutical Policies
circumcision (VMMC) for HIV prevention.
(EMP). The TAG reviews the clinical data on a specific product and advises the Department of EMP whether the evidence
Modelling studies indicate that national male circumcision
demonstrates that a specific device is efficacious in removal of
programmes will have the greatest public health impact in these
the foreskin and safe for use in the intended population. The
14 priority countries, averting up to 3.4 million HIV infections
Department of EMP assesses the product to see that it meets
through 2025, and will provide the largest cost-saving (USD
international standards (through a review of the product dossier)
16.5 billion) if services are scaled up rapidly. However, currently
and inspects the manufacturing site(s) to assess the adequacy
recommended surgical methods for adult male circumcision
and effectiveness of the manufacturer's quality management
involve considerable time and skill. Thus, innovations in the
system and the correct implementation of their documented
procedure, including male circumcision devices, have been under
study over the past few years.
By the end of 2012, three manufacturers had entered the PQ
In 2008 and 2009 initial consultations reviewed the landscape of
Programme; sufficient data was judged to be available on two
technologies for male circumcision. In 2010 the WHO established
devices—the ShangRing and PrePex. The TAG was, therefore,
a Technical Advisory Group on Innovations in Male Circumcision
convened in January 2013 to review all available data on these
(henceforth "the TAG") for the purpose of reviewing and
devices, to advise on the clinical evaluation component of PQ and
advising the WHO on innovations in male circumcision, including
highlight programmatic considerations in the use of each device
devices. The Framework for the clinical evaluation of devices for
and to advise on priority research needs.
declaration of interests
The objectives of the meeting were to:
At the beginning of the meeting, the WHO secretariat explained the reasons for the written and verbal declarations of interests
• update the TAG on the:
and summarized the pertinent interests that had been declared
– status of devices in the WHO PQ of Male Circumcision
in writing prior to the meeting. All participants were invited to
Devices Programme
declare verbally to the group any other conflicts, or potential
– device risk assessments and
conflicts, of interest. No other members stated any current or potential conflicts of interest that might affect their impartiality,
– development of guidance on use of devices and issues from
judgment or advice. Review of the declarations by the secretariat
the research that will inform the guidance.
and the TAG chairs identified no significant conflicts or potential
• review all available clinical research findings on two male
conflicts of interest that would disqualify or restrict participation.
circumcision devices for adolescents and adults, specifically the PrePex and the ShangRing, to inform prequalification
The primary types of potential conflicts were due to participants'
involvement on research teams that had or were currently
• advise the WHO on:
studying one or more devices, involvement in modelling studies and a declared advocacy of "cautious optimism in favour" of
– review of study requirements for clinical evaluation of
devices. One participant had been previously employed by a
devices of the same category;
company that worked on the development of male circumcision
– operational and programmatic considerations on use of
devices, two currently or previously worked on male circumcision
devices to be addressed in the guidance;
device technologies, and one worked with and currently consults
– additional technical innovations that WHO should assess,
for the Bill and Melinda Gates Foundation, which has supported
or should stimulate further development of, to improve
device development and research.
coverage and/or accelerate scale-up of male circumcision in priority countries; and
– priority research to further advance work on male
circumcision for HIV prevention.
meeting process and roles of participants
The TAG is comprised of international y recognized experts
including representatives of research institutes, clinical scientists,
statisticians, medical device regulators and programme managers
in the field. The TAG is composed of members and observers.
Members of the TAG are experts appointed because of their
expertise in the field and are involved in the formulation of
recommendations. Observers from col aborating partners with
an interest in expanding male circumcision programmes for HIV
prevention represent the perspective of their institutions as wel
as contribute their technical knowledge. Observers do not directly
participate in formulating the advice and recommendations
of the TAG. Given the nature of the meeting documents that
were reviewed, TAG participants agreed to strict standards of
confidentiality and submitted signed confidentiality agreements.
programme and tecHnical updates
wHo Hiv department progress during 2012 WHO also convened a small expert group to conduct a risk
and planned guidance
analysis of devices in mid-2012. The outputs of this exercise (see below) helped to identify key potential risks associated with use of devices. WHO is preparing guidance on the use of devices for
The WHO Secretariat provided programmatic updates on the
adolescent and adult VMMC for HIV prevention in accordance
work of the WHO HIV Department during 2012. WHO remains
with the WHO guideline review processes.
fully committed to identifying and assessing priority technical innovations in male circumcision, including devices that have
The conclusions of this TAG meeting will inform several guidance
the potential to:
products on devices and device use, in particular:
• make the male circumcision procedure safer, easier and quicker
• The WHO PQ Programme component on clinical safety and
than current methods;
efficacy of the ShangRing and PrePex devices. This is one
• facilitate more rapid healing and/or entail less risk of HIV
part of the full product review and contributes to the decision
transmission or acquisition in the immediate post-operative
whether or not to prequalify a particular device. A summary
report will be provided on the clinical evaluation of each specific device.
• be used safely by (mid-level) health-care providers with a
shorter period of training than required for conventional
• Programmatic and operational considerations in the WHO
surgical male circumcision; and
guidance on use of devices for adolescent and adult VMMC for HIV prevention.
• be more cost-effective for male circumcision scale-up than
standard surgical methods.
The WHO also sought inputs from the TAG on additional technical considerations, including a review of the clinical
Given that a number of devices were available on the market, the
evaluation requirements to demonstrate equivalent efficacy and
WHO, with the inputs of the TAG, had produced the following
safety of a similar product, further research to be catalysed, and
guidance products to inform evaluation and use of devices:
additional promising technologies that should be considered.
• Framework for clinical evaluation of devices for male
circumcision (1), which:
prequalification of male circumcision
– outlines the clinical pathway for assessing suitability of
a device, including the minimum requirement for WHO consideration of efficacy and safety (two comparative
The WHO PQ of Male Circumcision Devices Programme
studies in different settings and two field studies in settings
undertakes a comprehensive assessment of the applications
of intended use);
submitted by device manufacturers through a standardized procedure based on international best practices and WHO PQ
– lists ideal device characteristics and potential evaluation
requirements, which include three main components:
– provides suggestions for the stepwise introduction of a new
• Review of the application form with summary information
device, with scale-up in mind; and
about the product
– highlights regulatory considerations and the WHO
• Review of the product dossier, including review of clinical
• Use of devices for adult male circumcision in public health HIV
• Inspection of the manufacturing site(s).
prevention programmes: conclusions of the WHO Technical Advisory Group on Innovations in Male Circumcision (2), which
The role of the TAG in the PQ of Male Circumcision Devices
provided initial conclusions based on limited evidence on the
Programme process is review of the clinical safety and efficacy
use of the PrePex device in early 2012.
of the device based on clinical evidence generated within the clinical evaluation framework described earlier.
– As the data reviewed were from a series of three clinical
studies conducted in only one low-resource country
To date, three devices—namely the PrePex, ShangRing and
(Rwanda), the TAG concluded that additional studies were
AlisKlamp—have entered the WHO PQ Programme. The
needed before advice could be generalized beyond Rwanda.
manufacturer of a fourth device, the TaraKlamp, has expressed
During 2012 the WHO PQ of Male Circumcision Devices
interest but has not yet submitted an application. Review of the
Programme reviewed two device products and responded
PrePex device has moved the most swiftly through the stages
to requests from manufacturers of two other devices. More
of PQ and is the closest to meeting clinical evaluation and other
details on PQ are noted below. The link to the PQ documents
requirements. Once a product has been prequalified, it will be
included on a list of devices published on the WHO web site (see
above). This paves the way for procurement by UN agencies,
WHO Member States, donors and other interested purchasers.
or process) of the device to the PQ Programme. It is not the
Prequalification does not imply WHO approval to import or to use
manufacturer but rather the WHO programme that decides what
the device in any particular country, as this the prerogative and
constitutes a "significant" change in the design of the product or
responsibility of the national regulatory authorities.
the manufacturing process, and if a re-evaluation is needed.
The main points from discussions that followed these updates included:
technical update 1: risk analysis of male
• The steps in the PQ process require significant staff time and
financial resource investments.
The WHO held a technical consultation in Geneva, 6–7 August
– These financial resources have been provided by donors and
2012, to reach consensus on the classification scheme for male
the public sector, and the manufacturer is not charged by
circumcision devices and to conduct a risk analysis on of devices.
WHO for work performed for PQ of a product.
Three categories of in-situ devices (i.e. devices that remain in
– The process can take many months before the manufacturer
place for some period of time) for adolescent and adult male
satisfactorily meets requirements. It involves the
circumcision were agreed upon based on their mechanism of
manufacturer submitting complete documentation,
responding to requests for clarification, and implementing suggested corrective actions following WHO site inspections.
• Clamp, with subcategories: a) collar clamp (e.g. ShangRing); b)
• A PQ decision is time-limited. WHO will arrange for the
vice clamp (e.g. TaraKlamp)
products and manufacturing sites included in the WHO list
The mechanism of action consists of rapid, tight compression
of prequalified male circumcision devices to be reassessed
between hard surfaces to achieve haemostasis. Compression
at regular intervals. Prequalified diagnostic products are
is sufficient to prevent slippage of tissue such that the foreskin
reassessed usually every three to five years, or sooner if
can be removed at the time of, or soon after, application of
warranted, such as in the case of reports of product defects. If,
the device. Part or all of device is left in situ for more than 24
as a result of reassessment, it is found that a product and/or
hours. Injection with local anaesthesia is required.
specified manufacturing site no longer complies with the WHO
• Ligature compression (e.g. Plastibell for infants)
requirements, such products and manufacturing sites will be
The mechanism of action consists of a rapid, tight compression
removed from the list. Failure of a manufacturer to participate
between a hard surface and a non-rigid ligature that is tied to
in the reassessment procedure also will lead to removal from
hold the foreskin in place between the hard surface and the
the list. For prequalified devices the same principle will be
ligature. Compression is sufficient to achieve haemostasis and
applied, with re-inspection occurring sooner as indicated,
prevent slippage of tissue such that the foreskin can be removed
including for a new product and manufacturer.
at the time of, or soon after, application of the device. Part or
• A PQ decision can be retracted if concerns with safety are
all of the device is left in situ for more than 24 hours. Local
substantiated. Once a product is prequalified, International
anaesthesia is required. The compression force and the security of
Organization for Standardization (ISO) 13485 requires
the knot depend on the provider.
the reporting of serious adverse events and post-market
• Elastic collar compression (e.g. PrePex).
surveillance. Since national adverse event monitoring systems
The mechanism of action consists of slow compression
are often weak, the TAG urged the standardization of post-
between an elastic ring and a hard surface that is sufficient to
market surveillance and that countries improve the reporting of
occlude circulation and produce tissue ischaemia. Part or all
adverse events. PEPFAR will collaborate with WHO to support
of the device and the foreskin are left in place for more than
national programmes in post-market surveillance of the use of
24 hours, thereby causing ischaemic necrosis of the foreskin.
male circumcision devices.
The device and the foreskin are removed at a later date. Such
• The manufacturer must report, in addition to serious adverse
devices can be applied without the need for injected local
events, change(s) in the design or manufacturing (material
The consultation then used the Failure Modes and Effects Analysis
Tables 1 and 2 summarize the results of the risk analysis of two
procedure (FMEA) which is one of the techniques specified in
male circumcision device categories.
ISO 14971, the international standard for the application of risk management to medical devices, to systematical y analyze,
Some key points for programme introduction were noted. As
evaluate and propose control measures on use of devices.
devices are rolled out from study to field conditions and with
According to ISO 14971, the manufacturer is responsible for
broader use, more failures and failure modes can be expected
establishing, documenting and maintaining a continuous process
to occur. When the device is procured and used in a programme
of risk management/quality feedback for the lifetime of a device,
supported by a government or donor, it is more likely that
including identifying hazards associated with a medical device,
safety will be monitored through standardized serious adverse
estimating and evaluating the associated risks, control ing these
event (SAE) reporting than when it is procured and used by the
risks and monitoring the effectiveness of these controls. Feedback
private sector. User instructions are critical. Clinicians will need
information is obtained from the market in the form of customer
to be educated not to use devices that have not been clinically
complaints and proactive post-market surveil ance as well as
evaluated and are not prequalified. Devices that fail should be
internal y from production processes, if a problem is encountered
sent back to the manufacturer for analysis.
before the product or lot reaches the market.
The WHO consultation applied the FMEA technique to a device
technical update 2: clinical evaluation of
category: identifying failure modes associated with the specific
the prepex and the shangring devices
device category, quantifying the risk and identifying actions to mitigate risks. The exercise focused on device categories for use
The TAG conducted a detailed review of all available clinical
in adolescents and adults (rather than infants) and on those that
safety, efficacy and acceptability data on two male circumcision
had entered the WHO PQ Programme. The FMEA technique takes
devices for adolescents and adults, the ShangRing and the
into account three factors:
PrePex. Data on the safety and efficacy of the PrePex were available from eight studies conducted in three countries in
• potential severity of an outcome (consequence of the harm)
east and southern Africa (Rwanda, Uganda and Zimbabwe).
• frequency of occurrence (per client procedure) and
These studies included an initial safety and efficacy study, two
• detectability of any potential failure (ease with which the
randomized comparative trials, two completed field studies and
failure can be detected at time of deployment or while the
interim analyses from two ongoing field studies. Safety and
device is in situ).
efficacy data for the ShangRing included data from five studies conducted in three countries (Kenya, Zambia and Uganda). Data
Individual scores were assigned to each potential failure mode
from studies conducted in China were summarized (3–6), but
for each of the three factors, using a scale of 1 to 5. A total
the TAG decided these data were not directly relevant to the
risk score was calculated by multiplying the individual factor
population where the intervention is prioritized. In addition, it
scores (highest score possible risk score is 125). A risk score of
was not clear whether the version of the device used in these
25 or above was considered by the participants as a priority,
studies was the same as that used in the African studies.
warranting that actions to mitigate risk be identified. Such actions could be through:
• Provider instructions, warnings and contraindications on use• Client information on use• Specification of the device (in its design and/or the material(s)
• Process and quality controls in manufacturing


1. shangringThe ShangRing is produced by Wuhu Snnda Medical Treatment
Figure 1: The original design of the ShangRing is
Appliance Technology Co. Ltd, Wuhu City, China. It is a
shown at the top (7). The design used in the
minimal y invasive method for boys and adult men undergoing
African studies is shown at the bottom (8).
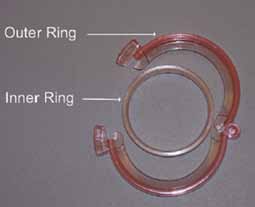
circumcision for phimosis or electively and was first described in the international literature in 2008 (7). The ShangRing is a col ar clamp circumcision type of device. The device consists of two concentric plastic rings that sandwich the foreskin of the penis. The mechanism of action consists of a rapid, tight compression of the foreskin between the hard surfaces to achieve haemostasis. The compression is sufficient to prevent slippage of tissue such that the foreskin can be removed at the time of device application. The device must be sterile. Anaesthetic injection is required.
The device is applied by placing the inner ring over the shaft of the penis at the height of the coronal sulcus. The foreskin is everted over the inner ring and then clamped in place and crushed by the outer ring. The foreskin distal to the device is then cut away. The device is removed at seven days by releasing the clamped outer ring, gently separating the inner ring from the healing wound, and then cutting the ring in two places to remove it from the shaft of the penis.
The original device used in China is shown on the top in Figure 1. It was available in different diameters, ranging from 13 mm to 40 mm in 2 or 3 mm increments. The device used in all the African studies is depicted at the bottom in Figure 1. It differed from the original design only with regard to the mechanism to secure the outer ring—the threaded locking mechanism in the original design was replaced with a ratchet that facilitated positioning and adjustment of the device over the everted foreskin. Also, the device was available in 26 mm to 40 mm diameter sizes in 1 mm increments. The correct device size is selected based on measurement of the penile circumference at the level of the coronal sulcus with a specially marked tape.
2. prepexTMThe PrePexTM is produced by Circ MedTech Limited in Israel.
Figure 2: The PrePex device
The device was specifically designed to be used by mid-level providers in resource-limited settings and to avoid the need for local anaesthesia during device placement. The device is an elastic collar compression type of device. It consists of an inner ring placed under the foreskin at the level of the coronal sulcus and an elastic O-ring that is aligned and released over the groove of the inner ring using an applicator (Figure 2). Blood flow to the foreskin is restricted by compression of the elastic ring on the inner ring, resulting in ischemia and necrosis of the foreskin. The device and necrotic residual foreskin are removed at seven days. Since there is neither cutting nor crushing of live tissue that would result in intense pain, there is no need for injectable local anaesthesia. The absence of bleeding means that there is no need for suturing and the device does not have to be sterile at the time of use.
process of evaluation of study data on
• Successful circumcision was defined as removal of sufficient
foreskin such that the coronal sulcus was visible with the penis in a flaccid (non-erect) state. Circumcision failures included clients who needed an additional intervention to complete the
retrieval of the evidence
circumcision and those with insufficient foreskin removed. The proportion of successful circumcisions was computed only on
In preparation for the TAG meeting, WHO staff searched
clients on whom the device was successfully placed.
the PubMed database for all published studies on the two
• Procedure time was computed for devices as the sum of the
circumcision devices and contacted investigators known to be
preparation and procedure times for placement and removal,
studying the devices in African countries. WHO staff reviewed
not counting the time period between the two. Times were
all published reports. Investigators made available to WHO
measured from start of the surgical procedure to completion of
secretariat confidential final reports from completed studies and
wound dressing (first to last touch) for conventional surgery or
interim reports from ongoing studies for review by the TAG. WHO
to end of device placement (last touch) for device application,
secretariat extracted key features of each study into a standard
but did not include the time for induction of anaesthesia,
format and compiled these to report the most important clinical
where used. Removal times were measured from first touch to
outcomes regarding safety and efficacy of the device in different
completion of wound dressing after device removal.
populations and in the hands of different providers. During the latter part of 2012, a subgroup of the TAG reviewed and
• Time to complete wound healing was defined as the number
commented on all data available. WHO sought clarifications from
of days from the date of conventional surgical circumcision
the study investigators where necessary.
or device placement (not from the date of intended or actual device removal) to the first date when complete wound
As the review of the clinical data by the TAG informs the
epithelialization was observed. Not all study teams used
development of guidance on use of devices, the process followed
identical definitions of complete wound healing, and the long
was similar to that recommended by the WHO Guideline
intervals between visits in some studies prevented a precise
Development Committee, including specifying outcomes of
estimate of the duration of healing.
interest. The evaluation criteria were in line with those identified
• Pain was measured in most studies using a Visual Analogue
in the Framework (1). External audits conducted either on
Score (VAS) with a range of 0–10, where 0 corresponds to "no
behalf of the study sponsor or by a team designated by the WHO
pain at all" and 10, to "worst pain imaginable", with clients
secretariat independently verified the quality of the research
shown pictograms for six different rating levels (Figure 3), with
study and the completeness of the data and reports.
text usually translated into the local language. Depending on the study and the follow-up schedule, the pain assessments
standardization of the priority outcomes
were made at specified time points, such as before or during device placement; specified times after placement; while
The TAG meeting evaluated the devices on the basis of the
wearing; before, during and after removal; and at selected
following critical outcomes and definitions:
follow-up visits. Additionally, some studies assessed the
• Eligibility for male circumcision with the device. All men
duration of the pain. Not all studies assessed pain at the same
must be screened for medical eligibility for circumcision, in
time points; the most comparable times have been selected
particular the absence of any penile abnormalities and current
in order to facilitate comparisons between devices and with
genital infections. For a particular device, use may be further
conventional surgical circumcision.
restricted due to: a) additional anatomical reasons, such as
Figure 3: Visual analogue pain scale and pictograms
phimosis (inability to retract the foreskin), a narrow foreskin opening or a short frenulum; or b) technical reasons that preclude device placement such as unavailability of a correct device size or inability to complete the device placement procedure. Therefore, device eligibility was defined as the proportion of men who met the criteria for conventional surgical circumcision, who were also eligible for circumcision with the specific device and in whom the device could be successfully placed.
definitions and classification of adverse events
• AEs resulting from insufficient or inadequate instructions for
use, deployment, implantation, installation, or operation, or
Although there had been attempts to standardize terminology
any malfunction of the investigational medical device; and,
and classification of adverse events (AEs) in studies of
• Any event resulting from use error or from intentional misuse
conventional male circumcision and circumcision devices, the
of the investigational medical device.
classification schemes evolved as more information about the types and timing of AEs became available. The different
In consideration of the above international definitions and the
mechanisms of action of the devices and the differences from
importance of ensuring a uniform classification that can be
conventional surgical circumcision techniques have led to
applied to clinical research on male circumcision, the WHO TAG
differences in the types of AEs and characterization of the AEs.
closely followed GHTF definitions and the following principles
This required that all observed AEs be reviewed and classified by
(for the two circumcision devices for which data were available
the TAG in a uniform manner. In doing so, the TAG was guided by
for review as well as other devices that may become available
internationally recognized principles and definitions of AEs and
with different mechanisms of action):
serious adverse events (SAEs).
• Any untoward medical occurrence, unintended disease or
The Global Harmonization Task Force (GHTF) (9) and the
injury, or untoward clinical signs (including an abnormal
International Organization for Standardization define an AE as:
laboratory finding) in subjects, users or other persons, whether
"Any untoward medical occurrence, unintended disease or injury,
or not related to the conventional surgical procedure or to the
or untoward clinical signs (including an abnormal laboratory
medical device used for performing or assisting in the male
finding) in subjects, users or other persons, whether or not
circumcision procedure was considered an AE.
related to the investigational medical device". This definition
• Any AE that was definitely not related to the circumcision
includes events related to the investigational medical device or
procedure or to handling or operating the medical device was
the comparator and events related to the procedures involved.
not considered further.
In addition, an SAE is defined as an AE that:
• Any AE that satisfied the GHTF definition of an SAE was
considered a serious adverse event (SAE).
1) led to a death; or,
• Any AE not classified as an SAE but that required an
2) led to a serious deterioration in the health of a patient, user,
intervention by a health care provider or medication
(parenteral, oral or topical) was considered a moderate AE.
a. resulted in a life-threatening illness or injury
• All other AEs were considered mild AEs. None of these events
b. resulted in a permanent impairment of a body structure or
would require any intervention.
In order to compile AEs over the different clinical studies and
c. required inpatient hospitalization or prolongation of
circumcision procedures, each AE was classified according to its
existing hospitalization
underlying cause or clinical presentation. It is important to note
d. resulted in medical or surgical intervention to prevent
that the classification adopted is designed to assess and compare
permanent impairment to body structure or a body function.
complications that occurred during the clinical research on male circumcision devices. While the overall principles underlying the
The International Organization for Standardization document
classification are likely to apply to programmes, the details will
14155 additionally defines an adverse device effect as an AE
have to be assessed for relevance in classifying AEs that occur in
related to the use of an investigational medical device, which
male circumcision programmes. Table 3 lists all AEs observed to
date according to category.
clinical evaluation of the shangring
Some clients with moderate or severe phimosis required a small dorsal slit to be made in the foreskin to facilitate eversion over
1.Overview of the studies
the inner ring (range across studies of 10%-28% of men).
The spontaneous detachment study showed that, if the device
The TAG reviewed clinical data on the safety, efficacy and
is not removed as scheduled at seven days, the device begins
acceptability of the ShangRing from studies conducted in China
to detach spontaneously and may come off without removal by
and three countries in Africa. Table 4 summarizes the studies
a medical provider. Partial detachments appear to be painful,
conducted in five sites in Africa (in Kenya, Uganda and Zambia).
cause discomfort as the partially detached device may snag and
Early studies in China demonstrated that the device was safe
cause tearing of tissue and bleeding. Therefore, the device should
when applied under local anaesthesia by skilled providers in
ideally be removed at seven days.
Chinese study participants (ages 5 to 95 years across studies), resulted in a neat and complete circumcision, and was potentially
faster and simpler than conventional surgical circumcision, as no
The overall mean placement time was 6.4 (SD 3.8) minutes,
suturing was required for haemostasis or wound closure. These
excluding the time for injection and induction of local
studies formed the basis for proceeding in a stepwise manner to
anaesthesia. The mean removal time was 3.1 (SD 1.8) minutes.
clinical research in African countries where public health male
The total of the mean placement and removal times (mean
circumcision programmes are being implemented.
10.3 minutes) was less than the mean procedure time in the
In its review of evidence, the TAG placed emphasis on the studies
randomized comparison with conventional surgery in Kenya and
conducted in the African region, which provided directly relevant
Zambia (mean 20.3 minutes).
information on the clinical performance of the device when
used in public health HIV prevention programmes: two initial safety and efficacy studies, two randomized controlled trials and
Adverse events in all the African ShangRing studies combined
two field studies. All the studies conducted in Africa with the
are summarized in Table 5. Based on a total of 1983 successful
ShangRing device used the same device design, which differed
device placements, there were:
from the original device only with regard to the mechanism to
• no SAEs—proportion 0.0% (95% confidence interval
secure the outer ring (see Figure 1). Safety and effectiveness
of the ShangRing device have been studied only in men age 18 years and older. There was consensus among the TAG members
• a total of 20 moderate adverse events—proportion
that the range and scope of the studies conducted on the
1.0% (0.6%-1.6%) and
ShangRing met the requirements set forth in the Framework.
• a total of 43 mild adverse events—proportion 2.2%
2. shangring study results
The ShangRing device is designed to avoid the need for haemostasis during surgery and to clamp the skin edges firmly
together to fuse as part of the healing process. Because of
The overall estimated proportion of clients eligible for
the tight clamping mechanism, local injectable anaesthesia
conventional male circumcision who were also eligible for
is required before device placement and then the foreskin
Shang Ring circumcision and in whom the device could be
is cut away distal to the device. The greatest proportion of
placed was 98.8%. The proportion of clients eligible for
moderate AEs was associated with pain during the anaesthetic
Shang Ring circumcision was 99.6%, due to a small number of
administration and device placement, requiring additional
clients excluded for minor foreskin abnormalities (e.g. short
medication for control in some instances, pain while wearing the
frenulum) that precluded device placement. These men could be
device, or partial device detachment or minor wound disruption
circumcised using a conventional surgical approach. Shang Ring
before device removal. Nevertheless, complications requiring
device placement procedures were started in 1998 clients and
intervention were rare (less than 1 in every 100 procedures).
were completed in all but 15 (99.2%) due to correct ring size not being available at the time of the procedure (8), the foreskin
It is important to note that the seven clients (0.4%) in whom
slipped from the outer ring (3), the foreskin was too short (1) or
the device placement procedure was started but could not be
damaged (2), or the outer ring could not be closed (1).
completed were all immediately converted to conventional surgical circumcision. Had facilities not been immediately
successful circumcision
available to safely complete the open circumcision (sterile field,
Circumcision was achieved in all clients on whom the device was
sutures or electrocautery for haemostasis and sutures for wound
successfully placed with the exception of three men (0.15%) who
closure), complications that would have resulted in serious
were considered to have insufficient skin removed.
adverse events might have occurred. A small number of wound disruptions occurred several weeks after device removal; these were clear departures from the normal healing process.
In the randomized controlled trial comparing ShangRing with
A person experienced in standard surgical circumcision must,
conventional surgery, there were no serious AEs, 2 moderate AEs
therefore, be available on site, together with appropriate
(both in the surgery arm) and 23 mild AEs (15 in the ring arm and
instruments and supplies.
8 in the surgery arm) in 197 ring placements and 198 surgical
• Circumcision using the ShangRing was demonstrated to be safe
circumcisions, P=0.40.
and successful in over 99% of clients.
• Healing is by secondary intention. It requires about one
Healing following male circumcision with the ShangRing device
week longer than after conventional surgery. The TAG
is by secondary intention and takes about one week longer
considered that there is a risk of HIV acquisition if men
than with surgery. In the comparative study, the mean time to
engage in unprotected sex before the wound is healed, but
complete healing was 44.1 (SD 12.6) days following ShangRing
the magnitude of risk is unknown. While this is also true of
placement compared with 38.9 (SD 12.6) days following surgery
circumcision by conventional surgery, because of the longer
(mean 5.2 days longer, 95% confidence interval 2.7–7.7 days).
healing time, the group stressed the importance of good
Thus, ShangRing circumcision requires a longer period of post-
counselling about sexual activity and condom use.
circumcision sexual abstinence than standard surgical methods.
• Adverse events associated with ShangRing procedures were
rare. In a total of 1983 successful device placements, there
were no deaths or serious adverse events (95% confidence
The ShangRing device requires injectable local anaesthesia
interval 0.0%–0.2%). The most common AEs were related to
before placement. The pain experienced during device placement
pain. All AEs were managed with, at most, minor intervention
and in the post-operative period is similar to that reported after
and resolved with no long-term sequelae. Although definitions
conventional surgery. Men reported some pain while wearing the
of serious and moderate AEs in the three randomized
device and a somewhat higher rate of pain during erection than
controlled trials that demonstrated the efficacy of male
at comparable times after conventional surgery. There is a risk
circumcision for HIV prevention in Kenya, South Africa and
of minor injury to the penis from the device itself and discomfort
Uganda are not directly comparable to those adopted in the
from catching or snagging the device while wearing it. Partial
device studies, the proportions are in a similar range—0.0%
detachment of the devices is associated with some discomfort
and pain, but this is rare if the device is removed as scheduled
• Phased implementation with careful monitoring and reporting
at seven days. There is short, transient discomfort and pain as
of device events and AEs is recommended in order to
the device is removed. In one study local anaesthetic spray was
better understand the frequency of technical failures of the
used prior to removal. This seemed to lessen but not completely
ShangRing and how best to manage such failures.
– Programmes must conduct active surveillance of the
Key points on the shangring made by the TaG
first 1000 clients to identify and record AEs based on
(Programmatic considerations are included in the next section).
standardized definitions. The active surveillance may change to passive surveillance after the first 1000 clients, if the
The TAG reviewed clinical data on the safety, efficacy and
incidence of events is reassuringly low as determined by
acceptability of the ShangRing device from five studies
independent review. Ongoing reporting of serious adverse
conducted in three African countries that resulted in device
events as part of post-market surveillance will need to be
placements on nearly 2000 men.
• The TAG considered the ShangRing to be clinically efficacious
• The TAG advised that the clinical studies necessary before
and safe for use in men 18 years and older, when the
a device is considered for prequalification by WHO per
procedure is performed by trained providers in public
the Framework for clinical evaluation of devices for male
health programmes. Skills and surgical facilities should
circumcision (2012) have been satisfactorily conducted.
be available to safely convert technical failures of device
• The evaluation, and thus advice on use, is currently limited to
placement to conventional procedures. The TAG recognizes
data on healthy males 18 years and older, as data were not
that this conclusion on clinical efficacy and safety is only one
available on men under 18 years or on men living with HIV.
component of the prequalification decision. The TAG based
• A small proportion of men were not eligible for device
its conclusion on the data currently available. This conclusion
use. Provision of or referral to conventional surgical male
must be reassessed in about one year as more experience with
circumcision would be needed. Some of the cases required
use of the device accumulates in diverse programmatic settings
immediate conversion to a conventional surgical circumcision.
outside the context of studies.
clinical evaluation of the prepex
2.0 (SD 0.8) minutes, placement procedure 1.5 (SD 1.0) minutes, removal preparation 0.4 (SD 0.2) minutes and removal procedure
1. Overview of the studies
2.0 (SD 1.1) minutes. In the two comparative studies, the mean total procedure time (placement preparation and procedure time and removal preparation and procedure time) was 5.7 (SD 1.4)
Table 6 summarizes the eight studies conducted in three
minutes compared with 19.2 (SD 3.9) minutes for conventional
countries, Rwanda, Uganda and Zimbabwe (interim analyses on
two ongoing field studies were included). The device was first clinically tested in Rwanda in a study that established the natural
history of the necrotic process in 50 volunteers. A second study investigated alternative forms of topical anaesthesia at the time
AEs occurred in 42 men in whom the device was successfully
of placement before a formal randomized comparison with the
placed (1.7%); the majority of AEs were mild or moderate,
dorsal slit conventional surgical approach was made. The next
while 9 (21%, or 0.4% of device placements) were considered
study to be completed was a field study in Rwanda in which
serious, as prompt surgical intervention was required to prevent
the device was placed and removed by trained nurses instead
potential serious long-term sequelae. The nine adverse events
of physicians. In order to comply with the requirements in the
categorized as serious resulted from device displacements during
sexual activity, masturbation, erection, possible placement
, a second series of studies was independently
error, or accidental dislodging by another person; early removals
conducted in Zimbabwe, starting with a small safety study
(including self-removals) secondary to pain; meatal injury at
followed with a randomized comparison and a second field study.
removal; and difficult removal due to necrotic tissue everted
2. prepex study results
over the elastic ring requiring surgical intervention, and wound dehiscence. Some of the displacements were associated with painful oedema, blistering and swelling as the blood flow
returned to the partially necrotic foreskin and required prompt
The overall estimated proportion of clients eligible for
surgical intervention to remove the foreskin and avoid serious
conventional male circumcision who were also eligible for PrePex
infection or injury to the penis. No mechanical device failures
circumcision and in whom the device could be successfully placed
were reported.
was 92.6%. The proportion of clients considered eligible for PrePex circumcision was 94.1%, due a number of clients excluded
for phimosis, narrow foreskin opening, tight frenulum, or small
Healing following male circumcision with the PrePex device is
wounds on the foreskin or penile shaft. PrePex placement
by secondary intention and takes about one week longer than
procedures were started in 2268 clients and were completed in
with surgery. In the comparative study in Rwanda, the mean time
all but 38 (98.3%) due to narrow foreskin opening (16), tight
to complete healing was 38.0 (SD 12.1) days following PrePex
or short foreskin (15) or adhesions (4), and three clients with a
placement compared with 23.0 (SD 7.5) days following surgery
penis circumference size outside the range of available ring sizes.
(mean 15 days longer, 95% confidence interval 12 to 18 days). In the comparative study in Zimbabwe, the difference in healing
successful circumcision
times was less pronounced, but interpretation of the data from
A total of 2417 PrePex devices were successfully placed in the
this study is limited by the absence of follow-up visits between
eight studies. For a large majority of clients (99.5%), the PrePex
days 7 and 42 post-procedure in the surgical circumcision arm.
circumcision was successful, leaving a neat circumferential
The overall mean healing time after placement recorded over
wound resulting in a final cosmetic appearance without suture
five studies was 42.3 days (standard deviation 7.8 days). Almost
marks. Circumcision had to be completed by conventional
all men healed by 8 weeks. Thus, healing following PrePex
surgery in a total of 12 clients (0.5%)—four removed the
circumcision requires a longer period of post-circumcision sexual
device themselves on Day 1 , two returned to the clinic on Day 2
abstinence than standard surgical methods.
requesting removal because of pain, discomfort or inconvenience, and in five clients the device became displaced on Day 1 (1), Day
2 (2), Day 4 (1) or Day 5 (1), following erection, masturbation,
The PrePex device does not require injectable anaesthesia
sexual intercourse or an assault. In one client surgery under local
during placement. Comparing the pain scores is difficult
anaesthesia was required to remove the band of necrotic foreskin
because the pain control protocols evolved as the studies
that had everted over the outer ring and prevented device
progressed and more information on pain became available.
In none of the studies was any injectable anaesthesia used for placement or removal of the PrePex device (excluding the
men with complications that required surgical intervention).
There was considerable variation in placement and removal
A topical anaesthetic cream containing 5% lidocaine was first
times over the different studies, with more experienced providers
introduced in the Rwanda field study and has been adopted in all
having lower procedure times. After the initial training and
subsequent studies.
familiarization process, mean placement preparation times were
Summary results of the VAS pain scores in the Rwanda studies
personal inconvenience wearing the device. Some of these
showed that pain at the time of ring placement was minimal. The
cases resulted in pain, rapid swelling and/or blistering of the
period of greatest discomfort and pain was in the 3–6 hours after
partially necrotized foreskin tissue, requiring urgent surgical
placement, with ischaemia induced by the device. Most study
intervention by a skilled surgeon in order to avert permanent
participants were provided with analgesics to take as needed at
disfigurement of the penis and/or severe local or systemic
home after placement; pain during the early ischaemic process
infection. In the studies conducted to date, appropriate
appeared to be adequately controlled in a large proportion of
surgical facilities have been available; all cases were
clients with readily available medications such as paracetamol or
successfully managed, with no long-term sequelae.
ibuprofen. There appears to be less pain while the device is worn
• Client instructions must clearly describe safe use of the device,
than at comparable times after conventional surgery, even during
symptoms that may develop with device displacement or early
erections. Study participants reported transient pain (short
removal as well as the possible serious outcomes and surgical
duration but quite severe) during device removal as the elastic
interventions that may be needed if instructions on abstinence
and inner rings were detached from the healing wound.
and wound care are not followed or if the device becomes
displaced (see next section).
Objectively assessing client acceptability in the early research
• The PrePex device was reportedly acceptable to a large
studies is difficult. However, a large proportion of clients
proportion of study participants. In contrast to conventional
expressed satisfaction with the aesthetic result. Pain, discomfort
surgical circumcision and other circumcision devices that
or user behaviour led to device displacements or early removals.
have been reviewed by the TAG, the PrePex device has the
Providers in at least three studies noted a strong odour in several
advantage of not requiring injectable anaesthesia or suturing
clients at the time of removal. Studies with the PrePex assessed
at the time of placement, thus requiring less time for the
loss of working days, which appeared to be fewer than following
procedures and causing less pain.
conventional surgery.
• PrePex providers must be appropriately trained to recognize
the potential serious complications that can occur if the
Key points on the prepex made by the TaG
device is displaced or removed early, and must ensure that
(Key programmatic considerations are noted in the next section.)
such clients are rapidly assessed for appropriate management (within 6–12 hours), including referral when necessary.
The TAG reviewed clinical data on the safety, efficacy and acceptability of the PrePex device from eight studies conducted
• If countries decide to introduce the PrePex device into their
in three countries with device placement on 2417 men.
public health programme, introduction should be done in a phased approach after the device is prequalified.
• The range and scope of these studies met the criteria
• Careful monitoring and reporting of AEs is necessary in order
established in the WHO Framework for clinical evaluation of
to better understand the frequency of device displacement and
devices for male circumcision.
self-removals and how risks can best be mitigated.
• The TAG advised that the clinical studies necessary before a
– Programmes must conduct active surveillance of the
device is considered for prequalification by WHO have been
first 1000 clients to identify and record AEs based on
satisfactorily conducted.
standardized definitions. The active surveillance may change
• Evaluation and any advice are currently limited to healthy
to passive surveillance after the first 1000 clients, if the
males 18 years and older, as the device has not yet been
incidence of events is reassuringly low as determined by
evaluated for use among younger ages or among men living
independent review.
• The TAG considered that there is an enhanced risk of HIV
• About 7% of clients eligible for conventional surgical
acquisition if men engage in unprotected sex before the wound
circumcision could not have the PrePex device placed for
is healed, but the magnitude of risk is unknown. Therefore,
various anatomical or technical reasons, including a narrow
the group stressed the importance of good counselling about
preputial opening or the correct device size outside range
sexual activity and condom use.
of five sizes produced. Circumcision was completed using
• The TAG considered the device to be clinically efficacious in
the PrePex in 99.5 % of clients on whom the device was
male circumcision and safe for use among healthy men 18
years and older when used by trained mid-level providers
• AEs occurred in 1.7% of clients; the majority were mild or
in public health programmes, provided that surgical backup
moderate. AEs in 0.4% were considered serious, and prompt
facilities and skills are available within 6–12 hours to
intervention was required to prevent potential serious long-
manage events that could lead to serious complications. This
conclusion is time-limited and must be reassessed in about one year as more experience with use of the device in diverse
• In a small number of clients (about 1 in every 200), the
programmatic settings is accumulated and reported.
device became displaced and /or was removed (including self-removal) due to client activities, pain, discomfort or
programmatic considerations in developing wHo
guidance on tHe use of male circumcision devices
During the course of the meeting and the session focused on
Considerations related to delivery site requirements that the TAG
programmatic considerations, the TAG noted the following key
identified included:
points. In general, evidence on devices is currently available from use in research conditions, in which many of the providers are
• The unique requirements of a device will need to be considered
highly skilled. As use expands and shifts from study populations
in the context of each type of service delivery site (e.g. fixed,
receiving "ideal care in well-resourced settings" to more real-
mobile, outreach, routine versus campaign).
world conditions, the TAG considered phased implementation
• At the initial introduction of a new device, it is advised to have
critical to determine the best and safest approaches for addition
both conventional surgery and device methods available.
of a new device method. Pilot studies are planned in a number
• A second visit is definitely required for device removal; services
of the priority countries. The information from these studies will
must be organized to meet the requirements of both visits.
further inform the use of the devices. Implementation plans must be tailored to the specific characteristics of each device.
• The type of surgical back-up skills and facilities must be clearly
specified, depending on device type, and available:
Clinical skills and competencies for device placement,
– "Immediate/on-site" surgical skills will be necessary at the
removal and management of AEs should be available within
time of ShangRing placement.
an ‘individual' and/or a ‘team'. For conversion to a surgical procedure after commencement of a device circumcision,
– "Within 6–12 hours timeframe" surgical skills must be
surgical staff may need skills beyond those needed to perform
available during the week that men have a PrePex device in
conventional surgical circumcision. Required clinical skills
situ, in case of an AE requiring urgent intervention.
and training will differ according to device. For example,
• Referral systems and contact numbers should be in place prior
ShangRing placement requires skills similar to those required for
to adding a device to any service.
conventional surgery, but more advanced skills and experience
• For men not eligible for a device (such as those under 18
are required to manage the rare cases when the ShangRing
years old or HIV-positive), service sites must determine if
placement procedure cannot be completed; these skills should be
conventional surgery is to be available on site or through a
available on site. The surgical intervention necessary after PrePex
functioning system of referral to services at another location.
device displacement or self-removal after the ischemic process has started requires a surgeon experienced with managing
• Programmes need to indicate pain management protocols for
swollen tissue and abnormal foreskin anatomy. These skills and
each specific device and for all stages of device use (pre-, in
facilities must be available or obtainable within 6 to 12 hours.
situ, at removal and post removal); these protocols must be
All providers must be knowledgeable and trained to manage
potentially life-threatening complications as well as the expected
Male circumcision is one essential component of the "minimum
and foreseeable side-effects.
package" of services, and all other components also must be available.
Information should be available for providers, including a
• Accurate messaging is needed on care and hygiene, possible
training manual and instructions for use of the device. The EMP
symptoms and management of device use, including the likely
Department stated that the evaluation of the manufacturer's
event of some pain. Symptoms such as pain, odour, bleeding
instructions for use (IFU) is part of the PQ programme. The
and swelling should be clearly described.
IFU should include pictures and step-by-step instructions from
• Clients must also be instructed on safe behaviours while the
beginning to end (placement and removal) and should list the
device is worn, including avoidance of sexual activity and
equipment that is provided in procedure package and additional
masturbation and the risks associated with such activity
accessories that are required. The TAG asked to review the
(with the PrePex risk of displacement, bleeding, swelling and
IFUs prior to a PQ decision. Considering the limits of any IFU,
ulceration and need for surgical circumcision).
programmes will still be responsible for the training and for developing manuals that will address specific issues such as
• If a device displaces or becomes dislodged, clients must know
pain management.
where to return to receive skilled surgical care or referral and transport arrangements to such care, within 6–12 hours.
Client counsel ing and education is an essential activity for good
There are a number of other issues that programmes will need to
clinical practice, informed consent and mitigation of risks related
consider prior to introduction and use of a device, including:
to client behaviours. Client instructions must clearly indicate the process and requirements of use of a specific device. Clients'
• The organization of the supply chain and logistics will be
partners should also be provided instructions. Points that should
needed. Multiple device sizes will be required and must be
be included in client instructions include the following:
sufficiently stocked through good supply management and forecasting. The choice of the correct device size is likely to be
• Once placed, a device must remain for seven days. In case
critical for avoiding adverse outcomes, but as yet the tolerance
a client desires to remove the device early, clients must be
margin for using a device one size too small or too large is not
instructed to return to the clinic. For the PrePex device early
removal would likely require a conventional surgery to safely complete the circumcision.
• Effective training and training materials will need to be
• Clients must understand that wound healing may take about
one week longer than following surgery, and that, until
• Sterility requirements and accessories required will need to be
complete healing, they should continue abstinence or use a
condom to protect the wound and reduce HIV transmission
• Regulations/policies will be needed on product approval in the
risk. Also, the nature and appearance of secondary healing
country and on which providers are permitted to perform male
should be described to men.
circumcision with a device.
• Post-market surveillance will need to be set up in a
standardized manner.
information gaps and needs
The TAG discussed research gaps that should be addressed in the
• As full healing and resolution of scarring may take up to one
near future. Over the next 12 months, PEPFAR and the Bill and
year, outcomes one year after circumcision is performed with
Melinda Gates Foundation will support pilot studies on the use
a device should be assessed to document long-term wound
of the ShangRing and the PrePex devices in VMMC programmes
healing and final cosmetic result.
in most of the countries in eastern and southern Africa. These
• Sizing studies are required, as the choice of the correct device
pilot projects wil have monitoring components, particularly the
size is likely to be critical for avoiding adverse outcomes.
monitoring and analysis of AEs, which will provide more data on their frequency and more detailed information on causes of serious
A brief update on ongoing/planned studies on the use of male
AEs, such as PrePex displacement or ShangRing device failures.
circumcision devices for infants such as AccuCirc compared with Mogen and Plastibell in Botswana, Zimbabwe and Uganda
The following additional gaps regarding the use of male
was provided by the WHO secretariat. TAG members expressed
circumcision devices were identified:
interest in moving forward infant circumcision, but WHO noted that due to limited resources the focus would be on review of
• Bridging studies are required to establish performance and
data when it becomes available.
safety in younger populations since neither the ShangRing nor the PrePex have been evaluated in men under the age of 18
addressing other technical issues
• Since there are limited data in HIV-infected adolescent males
Due to the limited time available, two items on the agenda were
and adult men, it is important to document the safety of the
device in such clients. Risk of HIV transmission during wound healing should be assessed through modelling studies to better
• review of the study requirements for clinical evaluation of
inform the consideration of risks and benefits.
devices in the same category;
• Studies are needed to assess the acceptability of the devices,
• advise on additional technical innovations that WHO should
particularly regarding the recommended period of sexual
assess or should stimulate further development of in order to
abstinence and the presence and management of pain, odour
improve coverage and/or accelerate scale-up of medical male
and urination problems while the devices are in situ.
circumcision in priority countries.
• More research is required to identify the best protocol for
The TAG will address these items through telephone and
managing pain at each point in the device use process.
electronic communications during the year.
• The frequency of SAEs in non-study settings needs to be
next steps
Key activities for the coming year include:
• Follow up with other technologies that have the potential
to accelerate public health male circumcision programmes,
• Complete the summary reports on the clinical performance of
specifically use of the Gomco clamp and surgical adhesive;
each device as part of the prequalification process;
• Collate and monitor the incidence of device-related SAEs
• Finalize the tables and summaries of adverse events
occurring in programmes and provide regular updates to the
and provide feedback to the study investigators on the
classifications adopted by TAG;
• Convene the next TAG meeting in early 2014 when sufficient
• Review the Instructions for Use submitted by the device
additional data on male circumcision devices used in
manufacturers in accordance with the TAG recommendations;
programmatic settings is available, and review the TAG
• Incorporate feedback from the TAG into the generic guidance
conclusions on the clinical performance of the PrePex and
on use of devices by the Guideline Development Group;
Shang Ring devices.
taBles
Table 1: Key risks of elastic col ar compression devices as
identified by WHO failure modes and risk analysis, August 2012
Potential failure
Instructions and
Clear and detailed
Untrained provider
Excessive blood loss
Penile strangulation
Training and user
Incorrect gauging
Insufficient foreskin
Device displacement
Excessive bleeding
Patient selection
Insufficient pressure
Matching components
Applied pressure
Septicaemic shock
O-ring properties
Properties of O-ring
Stress relaxation
Septicaemic shock
O-ring properties
Irritation and/or
Biocompatibility (ISO
Material for O-ring
Adverse reactions
Anaphylactic shock
10993)Specification and
Ring breaks after a
Damage to penis/glans
Properties of inner ring Inadequate strength
material testing at end
of shelf-life Device design
Local and systemic
Contact duration
Accumulation of debris Colonisation of device
Instructions for
Ulceration, pain
Information for patients
Inappropriate cleaning
Choice of materials
Patient instructions,
Reasonably foreseeable Intercourse
Device displacement
Bleeding, damage to
appropriate selection
misuse by patient
Self-removal of device Injury to self or partner penis, infection
of patients (user
Reasonably foreseeable Reuse of device
Damage to penis, glans Design of components
misuse by clinic or
Table 2: Key risks of clamp col ar devices as identified by WHO failure modes and risk analysis, August 2012
Potential failure
Instructions and
Clear and detailed
Untrained provider
Excessive blood loss
Inadequate sterilization
Potential infection
Sterilization validation
Packaging validation
Packaging breached
Potential infection
Seal integrity testing
Penile strangulation
Training and user
Incorrect gauging
Insufficient foreskin
Device displacement
Excessive bleeding
Patient selection
Irritation and/or
Biocompatibility (ISO
Material for O-ring
Adverse reactions
Anaphylactic shock
Failure after placement
Design verification
and foreskin removed
Product testingManufacturer's quality
Damage to penis,
management system
Outer ring too loose
Device displacement
and product inspection Instructions for useSpecification and
Ring breaks after a
Damage to penis, glans
Properties of inner ring Inadequate strength
materials testing at end
of shelf-life Set appropriate lower
Inadequate force
Excessive bleeding
Shock, blood loss,
limit for applied
Device displacement
Properties of outer
Ring breaks after 6–8
Excessive bleeding
Supplier evaluation
Inadequate strength
Testing and inspection
Local and systemic
Accumulation of debris Colonization of device
Instructions for clients
Ulceration, pain,
Information for clients
Inappropriate cleaning
Choice of materials
Patient instructions,
Bleeding, damage to
Reasonably foreseeable
Device displacement
appropriate selection
misuse by patient
Injury to self or partner
of patients (user
Self-removal of device
Reasonably foreseeable Reuse of device
Damage to penis, glans Design of components
misuse by clinic or
Table 3: Classification of serious, moderate and mild adverse events for review of clinical data on device safety by the WHO TAG, 2013
Serious adverse event
Required surgical intervention to prevent permanent impairment to a body structure
or a body function
Pain or discomfort resulting in early removal
Difficult removal
Wound disruption requiring suturing
Moderate adverse event
Required intervention or medication
Severe pain at time of, or soon after, device placement or surgery
Infection requiring medication
Pain or discomfort resulting in early device removal
Wound disruption
Difficult removal
Insufficient skin removed
Mild adverse event
Did not require intervention
Anaesthetic complication
Pain at time of, or soon after, device placement or the surgical operation
Displacement requiring repositioning
Bleeding or oozing (pressure and/or dressing)
Wound disruption
Partial detachment
Insufficient skin removed
Table 4: ShangRing clinical studies in Africa
Study [type of study]
Number and type of Type of providers
Safety Study (Kenya)
Homa Bay District Hospital, 40 healthy HIV-negative Physicians and nurses experienced in
[case series] (8)
conventional surgical circumcision
Spontaneous Detachment
Homa Bay District Hospital, 50 healthy HIV-negative Physicians and nurses experienced in
Study (Kenya) (10, 11)
conventional surgical circumcision
Randomized Comparison
Kenya: Homa Bay District
Non-physicians under supervision,
with Surgery (Kenya and
negative men (200
physicians and non-physicians, all with
Zambia) [comparative
Zambia: University
allocated to ShangRing, extensive experience with surgical male
trials] (12–14)
Teaching Hospital (UTH),
200 to conventional
circumcision (>500 surgical procedures
Field Studies (Kenya and
Kenya: seven sites in Homa 1256 healthy men
Non-physicians and physicians, all with
Zambia) [field studies]
extensive experience with surgical male
Zambia: Male Circumcision
Centre and UTH, Lusaka
Acceptability and Safety
Rakai Health Sciences
621 health HIV-negative Clinical officers in sterile conditions in
(Rakai) [field study] (17)
Programme, Kalisizo, Rakai men, 508 of whom
outpatient operating rooms
Table 5: Adverse Events in all Shang Ring studies combined
Type of Event
Number of device placements
Serious AEs
Moderate AEs
Pain placement (PAIN)
Pain leading to early removal (PREM)
Wound disruption (WNDD)
Insufficient skin removed (ISKR)
Anaesthetic complication (ANAE)
Pain placement (PAIN)
Partial detachment (DETD)
Wound disruption (WNDD)
Insufficient skin removed (ISKR)
Table 6: PrePex™ clinical studies in Africa
Study [type of study]
Number and type of client
Type of providers
(reference number)
Safety and Efficacy Rwanda
Kanombe District and
50 generally healthy HIV-
Physicians and nurse operators
[case series] (18)
Military Hospital,
Randomized Comparison of
Nyamata District
217 generally healthy men (144
Physicians and nurse operators
PrePex and Surgery Rwanda
allocated to PrePex, 73 allocated
[comparative trial] (19)
to dorsal slit surgery)
Pilot Study with Nurse
Kanombe District and
49 healthy HIV-negative men age Nurses
Providers Rwanda [case
Military Hospital,
Field Study with Nurse
Kanombe Military
666 generally healthy men
Lower cadre nurses with no
Providers Rwanda [field study] Hospital, Kigali,
previous experience of PrePex
Phase 1 Safety Study
53 HIV-negative men
Physicians (urologists,
Zimbabwe [case series] (23)
Hospital, Zimbabwe
general surgeons and general practitioners) and assistants (senior registered general nurses)
Phase 2 Randomized
240 HIV-negative men
Controlled Trial Zimbabwe
Hospital, Zimbabwe
[comparative trial] (24)Phase 3 Field Study Zimbabwe Harare, Kadoma and
641 HIV-negative men
Nurses with physician back-up
[field study] (25)
Field Study, Kampala, Uganda International Hospital 634 healthy men
Surgeons, medical officers,
[field study] (26)
clinical officers and nurses
Field Study, Rakai, Uganda
Rakai Health Sciences 187 HIV-negative men
[field study] (27)
Table 7: Adverse Events in all PrePex studies combined
Type of Event
Per cent [95% CI]
Number of circumcisions
Serious AEs
Displacement (DISP)
Premature removal (PREM)
Difficult removal (DIFR)
Wound disruption (WNDD)
Moderate AEs
Displacement (DISP)
Premature removal (PREM)
Difficult removal (DIFR)
Burn blisters (BLIS)
references
1. Framework for Clinical Evaluation of Devices for Male Circumcision. Geneva, World Health Organization, 2012.
2. Use of devices for adult male circumcision in public health HIV prevention programmes: conclusions of the WHO technical Advisory Group on
Innovations in Male Circumcision. Geneva, World Health Organization, 2012.
3. Cheng Y, et al. Adult male circumcision using the Chinese ShangRing: results of 328 cases and a recommended standard surgical protocol in
China. National Journal of Andrology, 2009, 15(7):584-592.
4. Yan B, et al. Circumcision with the Chinese ShangRing in children: outcomes of 824 cases [Article in Chinese, English abstract only]. Zhonghua
Nan Ke Xue [National Journal of Andrology], 2010, 16(3):250-253.
5. Peng YF, et al. Standardized male circumcision with ShangRing reduces postoperative complications: a report of 351 cases [Article in Chinese,
English abstract only]. Zhonghua Nan Ke Xue [National Journal of Andrology], 2011, 16(11):963-966.
6. Li HN, Xu J, Qu LM. ShangRing Circumcision versus comventional surgical procedues: Comparison of clinical effectiveness [Article in Chinese,
English abstract only]. Zhonghua Nan Ke Xue [National Journal of Andrology], 2010, 16(4):325-327.
7. Peng Y-F, et al. Clinical application of a new device for minimal y invasive circumcision. Asian Journal of Andrology, 2008, 10(3):447-454.
8. Barone MA, et al. The ShangRing device for adult male circumcision: A proof of concept study in Kenya. J Acquir Immune Defic Syndr. 2011;
57(1): e7-e12.
9. Study Group 5 of the Global Harmonization Task Force (GHTF). Reportable events during pre-market clinical investigations. GHTF, 2012
10. Barone MA, et al. Randomized trial of the ShangRing for adult male circumcision with removal at one to three weeks: delayed removal leads to
detachment. JAIDS Journal of Acquired Immune Deficiency Syndromes, 2012, 60(3):e82-e89.
11. The ShangRing: evaluation of healing at three time intervals and potential for spontaneous detachment [confidential statistical report and
tables, study #10214]. Durham, NC, USA, FHI 360, 2011.
12. Sokal DC, et al. Randomized control ed trial of the ShangRing versus conventional surgical techniques for adult male circumcision in Kenya and
Zambia (TUAC0404). Presented to the XIX International AIDS Conference, Washington, DC, 22-27 July, 2012, abstract TUAC0404
13. Sokal DC, et al. Randomized control ed trial of a minimal y invasive circumcision device, the ShangRing, versus conventional surgical techniques
for adult male circumcision: safety and acceptability [submitted for publication], 2013.
14. Comparison of the ShangRing with conventional surgical methods: a randomized control ed trial (RCT10220) [confidential statistical report and
tables]. Durham, NC, USA, FHI 360, 2012.
15. Sokal DC, et al. A field study of male circumcision using a minimal y-invasive device, the ShangRing, in routine clinical settings in Kenya & Zambia.
[Report to The Technical Advisory Group on Innovations in Male Circumcision, World Health Organization]. Durham, NC, USA, FHI 360, 2012.
16. A prospective observational study of male circumcision using the ShangRing in routine clinical settings in Kenya & Zambia [confidential
statistical report and tables, study #10278]. Durham, NC, USA, FHI 360, 2012.
17. Kigozi G, et al. The acceptability and safety of the ShangRing for adult male circumcision in Rakai, Uganda [submitted for publication], 2013.
18. Bitega JP, et al. Safety and efficacy of the PrePex device for rapid scale-up of male circumcision for HIV prevention in resource-limited settings.
JAIDS Journal of Acquired Immune Deficiency Syndromes, 2011, 58(5):e127-e134.
19. Mutabazi V, et al. HIV prevention: male circumcision comparison between a non-surgical device to a surgical technique in resource-limited
settings: a prospective, randomized, non-masked trial. JAIDS Journal of Acquired Immune Deficiency Syndromes, 2012, 61(1):49-55.
20. Mutabazi V, et al. One arm, open label, prospective, cohort field study to assess the safety and efficacy of the PrePex device for scale-up of
non-surgical circumcision when performed by nurses in resource-limited settings for HIV prevention. Presented to the XIX International AIDS
Conference, Washington, DC, 22-27 July, 2012, abstract TUAC0405
21. Mutabazi V, et al. One arm, open label, prospective, cohort field study to assess the safety and efficacy of the PrePex device for scale-up of non-
surgical circumcision when performed by nurses in resource-limited settings for HIV prevention [Submitted for publication], 2013.
22. Mutabazi V, et al. One arm, open label, prospective, cohort field study to assess the safety and efficacy of the PrePex™ device for scale up of
non-surgical circumcision when performed by nurses in resource limited settings for HIV prevention (Protocol RMC-03). 2012 January 10.
23. Tshimanga M, eta al. Evaluation of safety and efficacy of PrePex™ device for male circumcision in Zimbabwe. Phase I: device safety trial report.
Harare, Zimbabwe, Ministry of Health and Child Welfare, 2013.
24. Tshimanga M, et al. A randomized control ed trial comparing the PrePex™ device to forceps guided surgical circumcision for rapid scale-up of
male circumcision in Zimbabwe. Phase II: randomized trial report. Harare, Zimbabwe, Ministry of Health and Child Welfare, 2013.
25. Tshimanga M, et al. Evaluation of safety and efficacy of PrePex™ device for male circumcision in Zimbabwe. Phase 3: cohort field study on
safety and efficacy of the PrePex circumcision device when performed by nurses. Harare, Zimbabwe, Ministry of Health and Child Welfare, 2013.
26. Galukande M, et al. HIV prevention: safety study of a non-surgical device for adult male circumcision with no injected anesthesia in a non sterile
setting. Kampala, Uganda, International Medical Group, 2013.
27. Kigozi G. Acceptability and safety of the prepex device for male circumcision: Rakai (UO1 AI075115-0451). Kalisizo, Rakai, Uganda, Rakai Health
Sciences Program, 2013.
annex: meeting agenda
Day 1: Tuesday 29 January 2013
Time
Welcome and introductions
Objectives and expected outcomes, review of agenda
Roles of members and observers, declaration of interests
Session I: Brief updates
Chair: Tim Hargreave
WHO guidance on use of devices for male circumcision
Prequalification status of devices
Irena Prat
Session II: Technical updates
Tim Farley
Recapitulation of research available on male circumcision devices for
adolescents and adults
Bill Potter
Risk assessment of devices
Clinical studies–is there a need to review requirements?
Session III: ShangRing
Co-chair:Tim Hargreave
Detailed review of research findings
Tim Farley
Con't: review evidence
Tim Farley
Reception (WHO D building cafeteria)
Day 2: Wednesday, 30 January 2013
Time
Session III: ShangRing (cont'd)
Co-chair:Tim Hargreave
Tim Farley
Session IV: PrePex
Co-chair: Stephen Watya
Detailed review of research findings
Tim Farley
Con't: Review evidence
Tim Farley
Discussion (cont'd)
Day 3: Thursday, 31 January 2013
Time
Session IV: PrePex (cont'd)
Co-chair:Stephen Watya
Tim Farley
Session V: Implications for WHO Guidance on use of devices
Highlights of Day 1 & 2 to address guidance on use of devices: operational
and programmatic considerations, and recommendations
Doris Mugrditchian/
Session VI: Additional technical innovations and research
Co-chair: Steve Watya
Bridging studies and special safety studies
Other male circumcision technologies including Gomco and glue
For more information, contact:
World Health Organization Department of HIV/AIDS
ISBN 978 92 4 150563 5
20, avenue Appia 1211 Geneva 27 Switzerland
Source: http://www.mmcinfo.co.za/control/resources/who-technical-advisory-group-devices-1.pdf
[Litigation ADR Questionnaire – India] CIVIL LITIGATION accompanied by an outline setting out the entire 1. In what language(s) may court proceedings be conducted? What arrangements can be made for Pre-action measures may be in the nature of a translation/interpreter services? request to court for grant of temporary injunctions
I n f o r m a t i o n s m a t e r i a l v o m 1 7 . 0 1 . 2 0 0 8 Zysten, Fisteln und Co. Der 18. November 1686 war der aufregendste Tag im Leben des Chirurgen Charles-François Félix (1653-1703). Ein Jahr lang hatte sich sein Patient der von ihm vorge-schlagenen Operation seiner Analfistel verweigert. Nun reckte er ihm den After ent-gegen, bereit, einige schmerzhafte Schnitte zu ertragen, denn mit Betäubungsmitteln war es damals nicht weit her. Der Patient war Schmerzen gewöhnt, zeitlebens hatten ihn unzählige Leiden geplagt. Doch ein Misslingen dieser Operation, wo-