Levitra enthält Vardenafil, das eine kürzere Wirkdauer als Tadalafil hat, dafür aber schnell einsetzt. Männer, die diskret bestellen möchten, suchen häufig nach levitra kaufen ohne rezept. Dabei spielt die rechtliche Lage in der Schweiz eine wichtige Rolle.
Binkolkata.in
Epidemiology of Parkinson disease in the city of Kolkata, India: A
community-based study
S.K. Das, A.K. Misra, B.K. Ray, A. Hazra, M.K. Ghosal, A. Chaudhuri, T. Roy, T.K.
Banerjee and D.K. Raut
Neurology 2010;75;1362-1369
DOI: 10.1212/WNL.0b013e3181f735a7
This information is current as of October 15, 2010
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
Neurology® is the official journal of the American Academy of Neurology. Published continuouslysince 1951, it is now a weekly with 48 issues per year. Copyright 2010 by AAN Enterprises, Inc. All rights reserved. Print ISSN: 0028-3878. Online ISSN: 1526-632X.

Epidemiology of Parkinson disease in thecity of Kolkata, IndiaA community-based study
Objective: No well-designed longitudinal study on Parkinson disease (PD) has been conducted in
India. Therefore, we planned to determine the prevalence, incidence, and mortality rates of PD in
the city of Kolkata, India, on a stratified random sample through a door-to-door survey.
Method: This study was undertaken between 2003 to 2007 with a validated questionnaire by a
A. Chaudhuri, PhD
team consisting of 4 trained field workers in 3 stages. Field workers screened the cases, later
confirmed by a specialist doctor. In the third stage, a movement disorders specialist undertook
T.K. Banerjee, FRCP
home visits and reviewed all surviving cases after 1 year from last screening. Information on
death was collected through verbal autopsy. A nested case-control study (1:3) was also under-taken to determine putative risk factors. The rates were age adjusted to the World StandardPopulation.
Address correspondence andreprint requests to Dr. Shyamal
Result: A total population of 100,802 was screened. The age-adjusted prevalence rate (PR) and
Kumar Das, Department of
average annual incidence rate were 52.85/100,000 and 5.71/100,000 per year, respectively.
Neurology, Bangur Institute ofNeuroscience, Kolkata 700025,
The slum population showed significantly decreased PR with age compared with the nonslum
population. The adjusted average annual mortality rate was 2.89/100,000 per year. The relative
risk of death was 8.98. The case-control study showed that tobacco chewing protected andhypertension increased PD occurrence.
Conclusion: This study documented lower prevalence and incidence of PD as compared with Cauca-
sian and a few Oriental populations. The mortality rates were comparable. The decreased age-
specific PR among slum populations and higher relative risk of death need further probing. Neurology®
2010;75:1362–1369
GLOSSARY
AAIR ⫽ average annual incidence rate; AAMR ⫽ average annual mortality rate; CI ⫽ confidence interval; FSQ ⫽ family
screening questionnaire; ICC ⫽ intraclass correlation coefficient; IR ⫽ incidence rate; MD ⫽ movement disorder; NSSO ⫽
National Sample Survey Organization; OR ⫽ odds ratio; PD ⫽ Parkinson disease; PPS ⫽ parkinsonism plus syndrome; PR ⫽
prevalence rate; PRM ⫽ Poisson regression modeling; RR ⫽ relative risk; SP ⫽ secondary parkinsonism; VA ⫽ verbal autopsy.
The epidemiology of Parkinson disease (PD) has important public health and social implicationsand also provides etiologic clues. India is a multiethnic country with genetic diversity. Recentcross-sectional studies from India, besides the Parsis study, have shown lower age-adjusted preva-lence rates (PRs) of PD in comparison with predominantly Caucasian and a few Oriental popula-tions (table 1).1-11 In India, with an aging population and increased life expectancy, it is expectedthat the disease burden due to PD will be enormous, but there is no prospective study to estimate itsincidence and mortality. The incidence rates (IRs) in different countries vary from 1.5 to 20 per100,000 per year.12-20 The wide discrepancy in rates among different studies may stem from ethnic-ity, environmental factors, and varied methodology. Previous studies have shown that subjects withParkinsonism have a higher relative risk of death compared with nonparkinsonian subjects in thesame age range.14,21 The low PR in most of the Indian studies may be due to either lower incidenceor higher mortality or a combination of the two.
From the Bangur Institute of Neuroscience (S.K.D., A.K.M., B.K.R., T.R.), Kolkata; Institute of Post-Graduate Medical Education and Research(A.H.), Kolkata; Institute of Psychiatry (M.K.G.), Kolkata; Indian Statistical Institute (A.C.), Kolkata; National Neurosciences Centre (T.K.B.),Kolkata; and All India Institute of Public Health and Hygiene (D.K.R.), Kolkata, India.
Study funding: Supported by the Indian Council of Medical Research (SWG/Neuro/9/2001-NCD-I and SWG/Neuro/20/2005/NCD-I).
Disclosure: The authors report no disclosures.
Copyright Inc.

Frequency of Parkinson disease as reported by studies from India and abroad
Period of
rate (per 100,000)
rate (per 100,000)
102,557 (Rural and urban)
Caucasians 87,025
Abbreviations: CLS ⫽ case linkage study; DDS ⫽ door-to-door survey.
a To US 1960 population.
b To US 1990 population.
c To US 2000 population.
d To US 1970 population.
e To Japan 1990 population.
f Standard population not mentioned.
Therefore, we planned to undertake a
ered at least 1 year of residency in the area to avoid the float-
door-to-door survey on a large heterogeneous
ing population.
A validated family screening questionnaire (FSQ) was used
population in the metropolitan city of Kolk-
to detect cases of major neurologic illnesses. This was adminis-
ata, India, to determine the prevalence, inci-
tered to the head of the family by field workers.2 In cases of
dence, and mortality rates of PD. A nested
confused PD patients as determined from history and examina-
case-control study was undertaken to deter-
tion, spouses or reliable family members were interviewed. Thisquestionnaire also contained information on demography and
mine putative risk factors.
questions to detect cases with movement disorders (MDs) in-cluding PD, such as tremulous movement of head, arms, and
METHODS A prospective community-based study was con-
legs and speech and gait abnormalities. We added 3 more ques-
ducted to find subjects with PD through a 3-stage house-to-
tions to capture subjects with MDs.
house survey. The institutional Ethics Committee cleared the
Survey. In the first stage, field workers screened the sample for
proposal, and written informed consent was obtained before
the positive cases. The field doctor examined them, recorded the
clinical details, and verified randomly chosen 10% of screened
Sampling. The sampling strategy has been published else-
negative population in each block to detect the false-negative
where. The survey area was the municipal limits of the city of
cases. The clinical details of all positive cases were scrutinized by
Kolkata (erstwhile Calcutta) with an area of 185 km2 and popu-
a team of senior neurologists, including MD specialists, and a
lation of 4.58 million.3
consensus diagnosis was reached. Few subjects were examined
The sample was chosen from the whole city through selec-
either in the institute or at home for resolving any confusion. In
tion of stratified random National Sample Survey Organization
the third stage, 1 MD specialist revisited all houses of the diag-
(NSSO, India) blocks based on geographical location and dwell-
nosed cases after 1 year of completion of the initial survey for
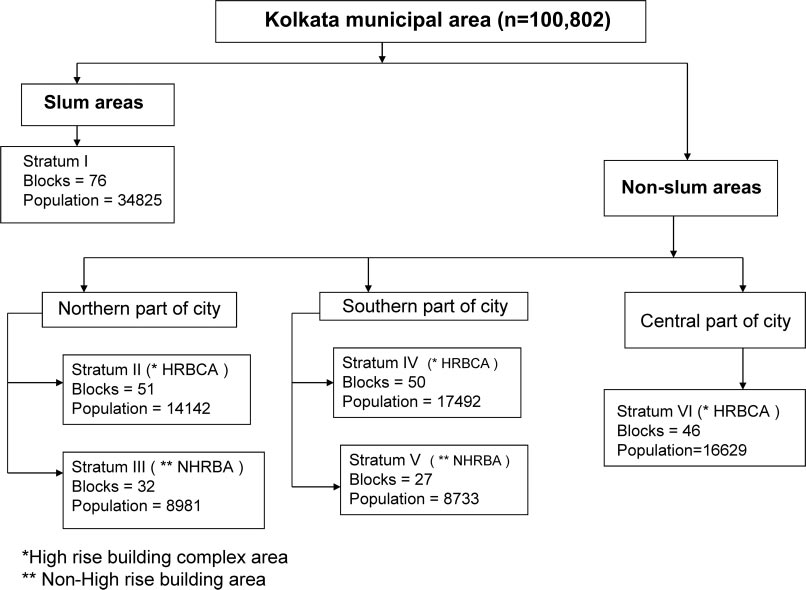
ings. The city population was initially divided into slum-
follow up and recorded any change in the clinical and treatment
dominant and non–slum-dominant areas. A total of 6 strata (1
profile, including death cases.
from slum areas and 5 from nonslum areas) were formed. The
In the initial phase, a study was conducted to determine the
slum population constitutes approximately one third of the In-
sensitivity and specificity of the screening questionnaire for PD
dian urban population. The slum dwellers are socioeconomically
in the MD clinic, where the specialist acted as the gold standard.
weaker and live in unhygienic, overcrowded conditions. Each
An initial cross-sectional survey was undertaken in 2003 to
stratum acted as a sampling frame (figure 1) from which a pro-
2004, and subsequently annual screening was performed be-
portionate number of NSSO blocks were selected by using ran-
tween 2004 and 2008 to find new cases and follow up with the
dom number tables. From each block, 50% of alternating
old cases. Verbal autopsy (VA) was performed in death cases.
families were surveyed. For purposes of inclusion, we consid-
This is a standard method of interview-based retrospective col-
Neurology 75 October 12, 2010

lection of information on death from a reliable family member or
of parkinsonism plus syndrome (PPS) and secondary parkinson-
close associate in the absence of a routine autopsy.22 All data
ism (SP) for diagnosis of PD. PPS was considered per defined
from VA cases were verified by the field doctor and subsequently
criteria.5 SP included those who had obvious causes leading to
by a senior doctor. The VA questionnaire was field tested to
features of parkinsonism, such as neuroleptic use in the past 6
determine sensitivity and specificity under the supervision of a
months preceding the onset of symptoms, infection, trauma,
senior doctor, who acted as the gold standard. The period for
stroke, and hydrocephalus.
prevalence was considered up to December 31, 2007, and inci-dence was calculated for the period between 2003 and 2007.
RESULTS The screened population was 100,802
Statistical analysis. PRs are expressed as per 100,000 popula-
individuals from 21,398 families out of 282 ran-
tion. Average annual incidence rates (AAIRs) and average annual
domly selected blocks. The literacy rate was 83.23%,
mortality rates (AAMRs) are expressed as per 100,000 popula-
and the sex ratio (men to women) was 1:1.12. A total
tion per year. Age-adjusted rates were calculated by adjustment
of 89 families refused or could not be contacted for
directly to World Standard Population.23 The 95% confidence
participation in the study. The total population was
intervals (CIs) of all the rates were calculated based on Poissondistribution. The 2 test was used to assess significance of differ-
exclusive of refusal cases.
ences in unpaired proportions; p ⬍ 0.05 was considered signifi-
The screening instrument for capturing PD cases
cant. A nested case-control study was undertaken with age (⫾5
showed a sensitivity of 88.23% (lower limit of 95%
years)–matched and sex-matched controls to assess the risk fac-
CI 63.09) and specificity of 100% (lower limit of
tors of PD. Controls were selected randomly from the case
95% CI 71.40) based on 40 clinic cases, and sensitiv-
neighborhood in a 1:3 (case-to-control) ratio, and 92% agreed to
ity and specificity of VA were 97.5% and 57.14%
participate (table e-1 on the Neurology® Web site at www.
neurology.org). Multivariate analysis of the case-control data was
based on 61 randomly selected community death
performed through conditional logistic regression. Poisson re-
gression modeling (PRM) was applied on prevalence and IR data
The intrarater validation of individual questions
to assess their relation with age and sex. Kaplan-Meier survival
on the FSQ showed perfect agreement among the 3
analysis was conducted with the prevalent cases of PD, the sur-
raters for all except 2 questions, which had an intra-
viving cases being censored at the time of study closure. Statistica
class correlation coefficient (ICC) value of 0.794, in-
versions 6 [StatSoft Inc., Tulsa, OK; 2001] and 17 [SPSS Inc.,Chicago, IL; 2008] were used for statistical analysis.
dicating strong agreement. In interrater validation,there was perfect agreement between raters in all but
Operational definition. To minimize the number of cases
3 questions. For 2 of these questions, agreement was
missed, the presence of at least 2 of the following features wasconsidered for parkinsonism: rest tremor, bradykinesia, rigidity,
strong (ICC 0.794), and for 1, it was fair (ICC
and postural instability.24 We excluded those cases with features
0.310) (details in table e-2).

Prevalence, incidence, mortality rates of Parkinson disease in Kolkata, India, and the corresponding
age-adjusted and sex-specific ratesa
Crude rate
M: 45.15 关26.77–71.38兴,F: 60.34 关37.95–91.15兴
4.56 关2.87–7.51兴
5.71 关3.59–9.40兴
M: 5.01 关2.50–8.96兴,
F: 6.20 关3.21–10.84兴
2.28 关1.21–3.80兴
2.89 关1.54–4.94兴
M: 2.65 关1.14–5.22兴,
F: 1.89 关0.60–4.34兴
a Figures in brackets denote corresponding 95% confidence intervals.
b Age-adjusted rate to Worlds Standard Population.
Table 2 shows the PR, AAIR, and AAMR of PD.
in table 4. PRM analysis of these results showed IR
Tables 3 and 4 depict age and sex distribution of the
increasing with age ( p ⬍ 0.001), but sex had no ef-
sample, which matched with the city population
fect ( p ⫽ 0.052).
(Census India, 2001).
Follow-up and mortality. In the third stage
Prevalence. Of 52 cases with parkinsonism, PD was
(follow-up visit), there were 13 deaths (8 men, 5
detected in 41 cases (the rest were PPS [6] or SP [5]).
women) of 41 cases over a period of 6 years, and a
Table 3 shows overall, age- and sex-specific, and age-
total of 3 cases could not be examined because of
adjusted PRs. By applying PRM, the PR rate showed
refusal (1) and migration (2). Of the remaining 25
a significant, but nonlinear increase with age ( p ⬍
cases, 1 case had multiple system atrophy, and an-
0.001) in comparison with sex ( p ⫽ 0.01). The mean
other had features of essential tremor. Thirteen sub-
age of the subjects was 62.03 years (range 28 – 82
jects were taking levodopa preparation and 9 other
years). Prior diagnosis was made in 23 cases
anticholinergics. Most of the subjects had shown a
(56.09%), and only 18 cases (43.90%) received
therapeutic response. None showed dyskinesia,
treatment. By applying PRM, the PR of the nonslum
but they received relatively low doses of levodopa.
population showed a significant increasing rate with
Additionally, 3 subjects were taking antipsychotics, 3
advancing age above 62.5 years compared with the
were taking antidepressants, and 4 were taking anti-
slum population.
hypertensives for comorbid disorders.
Incidence. A total of 23 cases of PD had onset of
Overall AAMR and sex-specific mortality are pro-
illness over the 5-year study period, and the AAIRs,
vided in table 2. The difference of AAMR between
age-adjusted rates, and sex-specific IRs are provided
slum (2.02) and nonslum (2.39) populations was in-
Age- and sex-specific prevalence of Parkinson disease in Kolkata, India
Age band, y
Total (95% CI)
33.83 (20.06–53.49)
46.23 (30.40–70.30)
40.67 (29.04–55.40)
AAR (95% CI)
45.15 (26.59–70.91)
60.34 (37.95–91.15)
52.85 (37.74–71.98)
Abbreviations: AAR ⫽ age-adjusted rate; CI ⫽ confidence interval; PR ⫽ prevalence rate.
Neurology 75 October 12, 2010

Age- and sex-specific incidence of Parkinson disease in Kolkata, India
Population cases AAIR
Population cases AAIR
Population cases AAIR
4.13 (2.06–7.39) 47,593
5.04 (2.61–8.80)
4.56 (2.87–7.51)
5.01 (2.50–8.96)
6.21 (3.21–10.49)
5.71 (3.59–9.40)
Abbreviations: AAIR ⫽ average annual incidence rate; AAR ⫽ age-adjusted rate (to World Standard Population); CI ⫽ confi-dence interval.
significant. Maximum mortality was observed in the
predictability was modest, with a Nagelkerke R2
70- to 74-year age band. The mean age of death cases
value at 0.137.
was 71.31 years (men: 70.38, women: 72.8). Thestandardized mortality ratio was 3.79 (95% CI 2.01–
DISCUSSION One concern about diagnosis of PD is
6.48; men: 5.23, women: 2.53). Thirteen cases of 31
the lack of biomarkers and dependence on clinical evi-
with PD and age greater than 55 years died, and over
dence. Epidemiologic ascertainment of cases is com-
the same period, 590 subjects of 12,683 nonparkin-
monly based on the administration of interview-based
sonian population died of other causes. So the rela-
questionnaires. Sensitivity and specificity of such ques-
tive risk (RR) stood at 8.98 (95% CI 5.89 –13.70).
tionnaires depends on the number of questions, and
The most probable causes of death were prolonged
various studies have shown that a minimum number of
bedridden state in 3 (23.07%), ischemic heart disease
questions (as low as 2) improves sensitivity but decreases
in 3 (23.07%), cerebrovascular accident in 2
specificity.25 Conversely, by increasing the number of
(15.38%), asthma in 2 (15.38%), train accident in 1
questions, specificity may be increased, but sensitivity is
(7.6%), sunstroke in 1 (7.6%), and cancer in 1
reduced. However, the lower limit of sensitivity and
(7.6%). The median survival time based on Kaplan-
specificity of the PD screening instrument indicates that
Meier survival analysis was 13.5 years (figure e-1).
a few cases might have been misdiagnosed or early cases
Case-control analysis. Both univariate and multivari-
might have been missed.
ate analysis were conducted to detect the association
The adjusted PR of PD in this study and those of
of risk factors of PD. Among controls, the preva-
other recently conducted studies from India1-3 have
lences of smoking and tobacco chewing were 33.3%
documented lower values as compared with Cauca-
and 26.08% among men and 0% and 20.37%
sian populations. A lower prevalence of PD has been
among women. In univariate analysis, history of reg-
shown among Bulgarian gypsies of presumably In-
ular tobacco use (besides smoking) showed a lower
dian origin in comparison with Caucasians living in
risk for development of PD (odds ratio [OR] 0.15,
the same environment.6 Similarly, an Anglo-Indian
95% CI 0.04 – 0.70), whereas hypertension increased
study from Southern India recorded a very low prev-
the risk (OR 2.45, 95% CI 1.03–5.84). The other
alence of PD.26 These 2 studies suggest a possible role
putative risk factors did not show appreciable in-
of genetic influence. Only the study among Parsis
crease or decrease in odds. In conditional logistic re-
from India observed high prevalence of PD, which
gression analysis, only nonsmoking tobacco use
can be explained by a distinct ethnicity and higher
showed up as a significant factor decreasing risk (ad-
aging population.13 Hence, lower prevalence among
justed OR 0.16, 95% CI 0.03– 0.75). The overall
Indian studies may be true and may be related to

either low incidence or increased mortality. The
tobacco chewing, similar to another report from In-
higher prevalence of PD among women has been
dia.32 The effect of tobacco chewing is prolonged be-
documented in Finland, Japan, and India.1,27,28 This
cause of persistent contact with buccal mucosa and
may be related to environmental factors rather than
provides higher potency than smoking cigarettes.33
genetic factors. Lack of estrogenic support was shown
The role of vascular pathology and that of hyperten-
to induce nigral cellular degeneration in animals.29
sion have been emphasized in vascular parkinson-
Because tobacco smoking was infrequent among
ism.34 However, hypertension is now considered as a
women in this study, the prevalence of PD may be
risk factor in neurodegenerative disorders such as
higher because of lack of its protective effect.30 How-
Alzheimer disease.35 Therefore, it is possible that hy-
ever, the lack of simultaneous increase of PR of PD
pertension may accelerate neurodegeneration. Con-
among the slum population compared with the non-
versely, a few cases of vascular parkinsonism also
slum population might indicate a protective effect
respond to levodopa.36 It is noteworthy that the inci-
due to some environmental factor, which needs to be
dences of hypertension and stroke are increasing in
probed further.
India,37 and some of the PD cases may be truly vascu-
This study documented a lower AAIR of PD as
lar in origin and probably misdiagnosed because of
compared with North American (20),14 many Euro-
levodopa responsiveness and lack of biomarkers em-
pean (19),15,16 Japanese (15),10 Australian (7),18 and
phasizing further study.
Chinese in Taiwan (10)9 populations, but similar to 1
Therefore, the lower prevalence of PD is explainable
Italian (10)16 and Libyan population (4.5)18 and higher
by lower IR, which may be related to either genetic or
than in the Chinese population (1.5).8 Age-specific
environmental factors. The studies from India have
AAIRs were also lower in comparison with similar stud-
documented a genetic contribution in up to 8.5% of
ies in the above populations.9,10,13–18 A meta-analysis by
cases of familial and sporadic PD.38 Thus, in the ab-
Zhang et al. showed that there was no change in IRs
sence of a genetic contribution, environmental factors
over the past 50 years, signifying that adjusted IR in this
may confer protection. Various phenolic compounds,
study is possibly stable.12 This study has shown no sig-
such as curcumin from turmeric, have shown antioxida-
nificant difference in sex-specific incidence and, hence,
tive and anti-inflammatory effects.39 Interestingly, Indi-
suggests that the chance of developing PD is almost
ans consume curcumin daily in their diet from
equal in both sexes. Conversely, evidence of 2-fold
early childhood. Curcumin prevents aggregation of
higher incidence among Italian men over women may
␣-synuclein in experimental animals and possibly cell
indicate a probable influence of sex in the occurrence of
death.40 It is possible that long-term consumption of
PD.31 The role of ethnic influence is revealed from dif-
curcumin might confer protection against development
ferent IRs among different racial populations, and the
of PD. This issue merits exploration.
lowest rate is noted among Asians.32 This is in accor-
There are some limitations in this study. Because
dance with our finding.
The AAMR of this study is comparable with those
the method of case ascertainment is interview based,
of studies worldwide, varying between 0.5 and 3.8 per
early cases may be missed. The lower 95% confi-
100,000.27 The higher mortality rate among men can
dence limit of sensitivity and specificity of the screen-
explain the higher prevalence among women. However,
ing instrument might indicate that a few early cases
the median survival time in this study is close to that of
may have been missed. Thus, the estimate could be
Taiwan.9 The causes of death in this study differ from
higher. Many elderly persons could not tell the exact
another Asian study where pneumonia was a com-
date of birth, and so lack of uniformity of age-
monly recognized cause of death among patients with
specific IRs and PRs may be related to misgrouping
PD. Also, a higher RR as compared with the United
of the subjects in different age bands. The diagnosis
States (2.2)21 and Taiwan (3.8)9 and standardized mor-
of PD is clinical, and some of the PD cases might be
tality ratio in this study (8.98) indicate either more se-
variants of PPS, if autopsy could be performed in
vere disease or a deficiency of health care in the
death cases. The case-control study has limitations,
community.8 Lack of a social support system and pau-
such as recall bias and improper quantification of the
city of trained manpower, rather than socioeconomic
exposure of interest. The specificity of VA is usually
factors, are the main constraints, because there was no
low because there is no way to validate the diagnosis
significant difference in mortality between slum and
in the absence of autopsy verification.22
nonslum cases. The earlier age at death is possibly a
Nevertheless, we have documented lower PRs and
reflection of the general pattern of mortality in individ-
IRs of PD. Mortality is comparable. In view of the close
ual countries, depending on life expectancy.
age and sex matching of our sample to the Kolkata pop-
The case-control study revealed that the only risk
ulation, the results are generalizable. The case-control
factor was hypertension and a protective factor was
study shows that PD increases with systemic hyperten-
Neurology 75 October 12, 2010

sion and decreases with tobacco chewing. The lower IR
Osuntokun BO, Adeuja AO, Schoenberg BS, et al. Neuro-
may be related to environmental factors. The higher RR
logical disorders in Nigerian Africans: a community-based
of death of subjects with PD demands greater attention,
study. Acta Neurol Scand 1987;75:13–21.
Zhang ZX, Roma´n GC. Worldwide occurrence of Parkin-
better care, and social support. Lack of a parallel in-
son's disease: an updated review. Neuroepidemiology
crease of PD prevalence among the slum population
might indicate the existence of a protective factor and
Bharucha NE, Bharucha EP, Bharucha AE, Bhise AV,
needs probing.
Schoenberg BS. Prevalence of Parkinson's disease in theParsi community of Bombay, India. Arch Neurol 1988;45:1321–1323.
Rajput AH, Offord KP, Beard CM, Kurland IT. Epidemi-
Statistical calculations were performed by Dr. A. Hazra.
ology of parkinsonism: incidence, classification and mor-tality. Ann Neurol 1984;16:278 –282.
MacDonald BK, Cockerell OC, Sander JW, Shorvon SD.
The incidence and lifetime prevalence of neurological dis-
The authors thank Dr. Mark Hallett, Director, Human Motor Control,
orders in a prospective community-based study in the UK.
National Institute of Neurological Disorders and Stroke, Bethesda, MD,for reviewing the manuscript and providing useful suggestions. The au-
Brain 2000;123:665– 676.
thors acknowledge the contribution of the task force members of the
Granieri E, Carreras M, Casetta I, et al. Parkinson's disease
Indian Council of Medical Research, New Delhi for neurologic disorders
in Ferrara, Italy, 1967 through 1987. Ach Neurol 1991;
for useful ideas, and the people of Kolkata as well as field staff for great
48:854 – 857.
cooperation. The authors also thank Prof. Prabir Burman, Professor of
Rosati G, Granieri E, Pinna L, et al. The risk of Parkin-
Statistics and Graduate Advisor, Department of Statistics, University of
son's disease in Mediterranean people. Neurology 1980;
California, Davis, CA, for valuable opinions about statistical calculation.
30:250 –255.
Jenkins AC. Epidemiology of parkinsonism in Victoria.
Received August 25, 2009. Accepted in final form June 24, 2010.
Med J Aust 1966;2:496 –502.
Ashok PP, Radhakrishnan K, Sridharan R, Mousa ME.
Epidemiology of Parkinson's disease in Benghazi, North-
Saha SP, Bhattacharya S, Das SK, Maity B, Roy T, Raut
East Libya. Clin Neurol Neurosurg 1986;88:109 –113.
DK. Epidemiological study of neurological disorders in a
Wang YS, Shi YM, Wu ZY, He YX, Zhang BZ; for Coor-
rural population of Eastern India. J Indian Med Assoc
dinational Group of Neuroepidemiology PLA. Parkinson's
2003;101:299 –300, 302–304.
disease in China. Chin Med J (Engl) 1991;104:960 –964.
Gourie-Devi M, Gururaj G, Satishchandra P, Sub-
Bennett DA, Beckett LA, Murray AM, et al. Prevalence of
bakrishna DK. Prevalence of neurological disorders in
parkinsonian signs and associated mortality in a community
Bangalore, India: a community-based study with a com-
population of older people. N Engl J Med 1996;334:71–76.
parison between urban and rural areas. Neuroepidemiol-
Soleman N, Chandramohan D, Shibuya K. Verbal au-
topsy: current practices and challenges. Bull World Health
Das SK, Biswas A, Roy T, et al. A random sample survey
Organ 2006;84:239 –245.
for prevalence of major neurological disorders in Kolkata.
Ahmad O, Boschi-Pinto C, Lopez AD, Murray CJL,
Indian J Med Res 2006;124:163–172.
Lozano R, Inoue M. Age Standardization of Rates: A New
de Rijk MC, Breteler MM, Graveland GA, et al. Preva-
WHO Standard. Geneva: World Health Organization;
lence of Parkinson's disease in the elderly: the Rotterdam
2000. GPE Discussion Paper Series No. 31.
Study. Neurology 1995;45:2143–2146.
de Rijk MC, Rocca WA, Anderson DW, Melcon MO,
Morgante L, Rocca WA, Di Rosa AE, et al; for The Sicilian
Breteler MM, Maraganore DM. A population perspective
Neuro-Epidemiologic Study (SNES) Group. Prevalence of
on diagnostic criteria for Parkinson's disease. Neurology
Parkinson's disease and other types of parkinsonism: a
door-to-door survey in three Sicilian municipalities. Neu-
Mutch WJ, Smith WC, Scott RF. A screening and alerting
questionnaire for parkinsonism. Neuroepidemiology
Milanov I, Kmetski TS, Lyons KE, Koller WC. Prevalence
1991;10:150 –156.
of Parkinson's disease in Bulgarian Gypsies. Neuroepide-
Ragothaman M, Murgod UA, Gururaj G, Kumaraswamy
miology 2000;19:206 –209.
SD, Muthane U. Lower risk of Parkinson's disease in an
Melcon MO, Anderson DW, Vergara RH, Rocca WA.
admixed population of European and Indian origins. Mov
Prevalence of Parkinson's disease in Junín, Buenos Aires
Province, Argentina. Mov Disord 1997;12:197–205.
Goldberg ID, Kurland LT Mortality in 33 countries from
Wang SJ, Fuh JL, Teng EL, et al. A door-to-door survey of
diseases of the nervous system. World Neurol 162;3:444 –
Parkinson's disease in a Chinese population in Kinmen
[published erratum appears in Arch Neurol 1996;53:508].
Kimura H, Kurimura M, Wada M, et al. Female prepon-
Arch Neurol 1996;53:66 –71.
derance of Parkinson's disease in Japan. Neuroepidemiol-
Chen RC, Chang SF, Su CL, et al. Prevalence, incidence,
and mortality of PD: a door-to-door survey in Ilan
Miller DB, Ali SF, O'Callaghan JP, Laws SC. The impact
County, Taiwan. Neurology 2001;57:1679 –1686.
of gender and estrogen on striatal dopaminergic neurotox-
Kusumi M, Nakashima K, Harada H, Nakayama H, Taka-
icity. Ann NY Acad Sci 1998;844:153–165.
hashi K. Epidemiology of Parkinson's disease in Yonago
Behari M, Srivastava AK, Das RR, Pandey RM. Risk fac-
City, Japan: comparison with a study carried out 12 years
tors of Parkinson's disease in Indian patients. J Neurol Sci
ago. Neuroepidemiology 1996;15:201–207.
2001;190:49 –55.
Baldereschi M, Di Carlo A, Rocca WA, et al; for ILSA
Zijlmans JC, Katzenschlager R, Daniel SE, Lees AJ. The
Working Group. Italian Longitudinal Study on Aging Par-
L-dopa response in vascular parkinsonism. J Neurol Neu-
kinson's disease and parkinsonism in a longitudinal study:
rosurg Psychiatry 2004;75:545–547.
two-fold higher incidence in men. Neurology 2000;55:
Das SK, Banerjee TK, Biswas A, et al. A prospective
1358 –1363.
community-based study of stroke in Kolkata, India. Stroke
Van Den Eeden SK, Tanner CM, Bernstein AL, et al. Inci-
2007;38:906 –910.
dence of Parkinson's disease: variation by age, gender, and
Biswas A, Gupta A, Naiya T, et al. Molecular pathogenesis
race/ethnicity. Am J Epidemiol 2003;157:1015–1022.
of Parkinson's disease: identification of mutations in the
O'Reilly EJ, McCullough ML, Chao A, et al. Smokeless
Parkin gene in Indian patients. Parkinsonism Relat Disord
tobacco use and the risk of Parkinson's disease mortality.
2006;12:420 – 426.
Mov Disord 2005;20:1383–1384.
Sun AY, Wang Q, Simonyi A, Sun GY. Botanical phenolics
Turnbull C. Vascular parkinsonism: an important update.
and brain health. Neuromolecular Med 2008;10:259 –274.
Age Ageing 2005;34:97–98.
Pandey N, Strider J, Nolan WC, Yan SX, Galvin JE. Cur-
Skoog I, Gustafson D. Update on hypertension and Alz-
cumin inhibits aggregation of alpha-synuclein. Acta Neu-
heimer's disease. Neurol Res 2006;28:605– 611.
ropathol 2008;115:479 – 489.
The AAN Provides a New Resource for Your Patients
Written by Ronald DeVere, MD, Director of the Taste and Smell Disorders Clinic in Austin, Texasand Marjorie Calvert, Food Consultant at the clinic, Navigating Smell and Taste Disorders includescauses, treatment options, and 36 recipes and additional tips that will make food appealing again.
"More than 200,000 people visit doctors each year for smell and taste problems, which often are thefirst sign of neurologic disorders, such as Alzheimer's disease, Parkinson's disease, head injury, ormultiple sclerosis," said DeVere.
"An enlightening guide. . this patient-oriented approach should be hailed as a groundbreakingbook. It is highly recommended for any patients suffering from these often undiagnosed and un-treated disorders and the relatives who help care for them."—Alan R. Hirsch, MD, neurological director at the Smell and Taste Treatment and ResearchFoundation in Chicago
Invite your patients to visit www.aan.com/view/smellandtaste for more information about this invalu-able resource. Available from all major booksellers.
Neurology 75 October 12, 2010
Epidemiology of Parkinson disease in the city of Kolkata, India: A
community-based study
S.K. Das, A.K. Misra, B.K. Ray, A. Hazra, M.K. Ghosal, A. Chaudhuri, T. Roy, T.K.
Banerjee and D.K. Raut
Neurology 2010;75;1362-1369
DOI: 10.1212/WNL.0b013e3181f735a7
This information is current as of October 15, 2010
including high-resolution figures, can be found at:
& Services
Supplementary material can be found at:
Subspecialty Collections
This article, along with others on similar topics, appears in the
following collection(s):
Parkinson's disease/Parkinsonism
http://www.neurology.org/cgi/collection/parkinsons_disease_parki
Prevalence studies
Risk factors in epidemiology
Permissions & Licensing
Information about reproducing this article in parts (figures, tables)or in its entirety can be found online at:
Reprints
Information about ordering reprints can be found online:
Source: http://binkolkata.in/wp-content/uploads/Neurology-_PD_ICMR.pdf
Painkillers can bring relief to people who are suffering from pain when taken as directed. However, the dangers of misuse must also be highlighted. Many painkillers are available over-the- effects such as drowsiness. This is why it counter (OTC) from pharmacies and is so important to read the information A huge market exists for painkillers and it shops without the need for a
Victoria Government Gazette No. S 108 Tuesday 25 June 2002 By Authority. Victorian Government Printer Transport Act 1983 ORDER AS TO DECLARED DRUGS I, Peter Batchelor, acting under section 93(1AA) of the Transport Act 1983, by this each of the substances specified in the Schedule to this Order; and (ii) any natural principle, any natural or