Levitra enthält Vardenafil, das eine kürzere Wirkdauer als Tadalafil hat, dafür aber schnell einsetzt. Männer, die diskret bestellen möchten, suchen häufig nach levitra kaufen ohne rezept. Dabei spielt die rechtliche Lage in der Schweiz eine wichtige Rolle.
Cesp-2016.vjf.inserm.fr

This article appeared in a journal published by Elsevier. The attached
copy is furnished to the author for internal non-commercial research
and education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling or
licensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of the
article (e.g. in Word or Tex form) to their personal website or
institutional repository. Authors requiring further information
regarding Elsevier's archiving and manuscript policies are
encouraged to visit:

Author's personal copy
Drug and Alcohol Dependence 112 (2010) 239–246
Contents lists available at ScienceDirect
Drug and Alcohol Dependence
Effect of the threat of a disulfiram–ethanol reaction on cue reactivityin alcoholics夽,夽夽
Marilyn D. Skinner a,b,c,d,∗, Mathieu Coudert b,e, Ivan Berlin b,e, Elodie Passeri b,g,Laurent Michel a,b,c,d, Henri-Jean Aubin b,c,d,f
a Centre Hospitalier Emile Roux, Centre de Traitement des Addictions, Limeil-Brévannes, Franceb Assistance Publique-Hôpitaux de Paris, Paris, Francec Inserm U669, Paris, Franced Université Paris-Sud and Université Paris Descartes, UMR-S0669, Paris, Francee Centre Hospitalier Universitaire Pitié-Salpêtrière, Paris, Francef Centre Hospitalier Universitaire Paul Brousse, Villejuif, Franceg Hôpital Mondor, Créteil, France
Rationale: Little is known about the effect of disulfiram on subjective and autonomic nervous system cue
Received 23 January 2010
reactivity in the laboratory. The dissuasive psychological effect manifested as a threat would seem to
Received in revised form 28 June 2010
prevail over the pharmacological effect.
Accepted 28 June 2010
Objectives: The primary objective was to determine whether there was a difference in cue reactivity
Available online 13 August 2010
responses during a threat condition compared to a neutral condition during alcohol cue exposure.
Methods: In a crossover randomized study, participants received threat and neutral messages during two
cue exposure sessions. The threat condition consisted of leading the patients to believe they had ingested
500 mg of disulfiram and the neutral condition of informing them that they had ingested a placebo, while
in both condition they received the same placebo.
Results: Physiological cue reactivity was demonstrated by a decrease in diastolic blood pressure during
Alcohol dependence
the threat compared to the neutral condition (p = 0.04). Heart rate and subjective cue reactivity measuresremained unchanged. There was a negative affect (assessed by the Positive and Negative Affect Scale) bycondition by exposure interaction.
Conclusions: The threat of a disulfiram–ethanol reaction appears to affect cue reactivity physiologicallyrather than subjectively. While the data does not show changes in subjective ratings, it is possible thatthere are alternative beneficial effects arising from other cognitive processes that are not captivatedby self-reported craving scales, reflected by decreases in negative affect and blood pressure. From thisperspective, disulfiram might be recast to be more acceptable to patients.
2010 Elsevier Ireland Ltd. All rights reserved.
and Berridge, 2008), but it nonetheless affects behavior that maylead to relapse. One method to reinforce abstinence has been to
One of the major challenges in addiction treatment is how to
increase aversion to alcohol. Disulfiram appears to help increase
prevent relapse when a patient desiring abstinence is thrown off
the duration of abstinence in patients who observe their treatment
balance by a reaction to alcohol or an alcohol related stimulus
schedule (Chick et al., 1992; Fuller and Gordis, 2004; Diehl et al.,
(Skinner and Aubin, 2010). This phenomenon may or may not be
2010; Mutschler et al., 2010). Furthermore, there is some evidence
identified as "craving" as it may occur without awareness (Robinson
that disulfiram decreases craving (De Sousa, 2004, 2005; Petrakiset al., 2005; De Sousa et al., 2008), but its mechanism of action oncraving is unclear.
Three studies evaluated subjective craving in order to com-
Additional materials are available with the online version of this article at
pare the effectiveness of disulfiram to acamprosate (De Sousa,
夽夽 Trial Registry Name: ClinicalTrials.gov identifier NCT00372749 on September
2005), naltrexone (De Sousa, 2004), and topiramate (De Sousa et
al., 2008). Disulfiram was found to reduce craving in alcoholics
∗ Corresponding author at: Centre de Traitement des Addictions, Centre Hospi-
post-treatment as measured by the OCDS (Obsessive Compulsive
talier Emile Roux, 1 avenue de Verdun, 94456 Limeil-Brévannes, France.
Drinking Scale) (Anton et al., 1995), but not to the same extent as
Tel.: +33 1 45 95 84 09; fax: +33 1 45 95 83 90.
E-mail address: [email protected] (M.D. Skinner).
the other medications. Disulfiram was found superior, however, in
0376-8716/$ – see front matter 2010 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.drugalcdep.2010.06.011
Author's personal copy
M.D. Skinner et al. / Drug and Alcohol Dependence 112 (2010) 239–246
reducing the number of drinking days. This may have been due
would interact with negative affect and cue reactivity. Demonstrat-
to the strong psychological effect of the prohibition of drinking
ing differences could impact the way physicians present disulfiram
on craving but also due to the association between disulfiram and
to potential patients.
reduced anxiety as Petrakis et al. (2005) have shown. On the other
We hypothesized that cue reactivity to alcohol would be affected
hand, it is still not clear if other cognitive or physiological processes
as follows: (1) the threat of a disulfiram–ethanol reaction would
were responsible for the superiority of disulfiram.
reduce the subjective desire to drink, and (2) heart rate and blood
In a large, randomized trial with alcohol dependent patients
pressure would be higher in the neutral condition than in the threat
with a comorbid DSM-IV, Axis 1 psychiatric disorder, the effective-
condition because of the increased risk of consuming in the neutral
ness of four different treatment conditions was compared over a
12-week period: a placebo alone, disulfiram + (blinded) naltrexone,
Secondary exploratory hypotheses were: (1) subjective craving
naltrexone alone, and disulfiram + (blinded) placebo (Petrakis et al.,
and physiological responses would not be correlated, (2) desire and
2005). The medication-alone groups had fewer drinking days com-
aversion would vary independently in both threat and neutral con-
pared to the placebo group; the combination treatment, however,
ditions, (3) compared to the less dependent participants, the more
did not have superior results in reduced drinking days or craving
dependent would have higher craving as well as higher heart rate
than either medication alone. Interestingly, the disulfiram patients
and blood pressure, and (4) negative affect would be associated
reported less craving based on the OCDS and fewer anxiety-like
with craving in both threat and neutral conditions.
symptoms than the naltrexone patients. Both groups also had sim-ilar compliance rates, probably because they were highly motivated
2. Methods
(Petrakis et al., 2005).
2.1. Participants
In another study, disulfiram was shown superior to acamprosate
and naltrexone in reducing drinking and probably craving because
Participants were recruited from inpatients in a French detoxification program
patients were told to target use of the medications to craving sit-
at Emile Roux Hospital, Limeil-Brévannes between November 2006 and September2008. Inclusion criteria were: (a) age 18 or older; (b) current diagnosis of alcohol
uations during the unsupervised phase of the study (Laaksonen et
dependence according to DSM-IV criteria (American Psychiatric Association, 1994);
al., 2008). No physiological measures were taken, raising questions
(c) abstinence goal of at least 6 months post-treatment; (d) intellectual, social, or
as to how disulfiram functions.
educational level sufficient to respond to the questionnaires; (e) no prior use of
The present study was conducted to address some of the gaps
disulfiram; (f) no contraindication to disulfiram; (g) no use of antidepressants or
in knowledge about the effect of a threat of a disulfiram–ethanol
neuroleptics during the past 6 days; (h) no treatment by naltrexone, acamprosate,beta-blockers, or clonidine during the past 7 days; (i) no use of benzodiazepines
reaction vs. a neutral condition on subjective and autonomic ner-
during the past 3 days except diazepam, maximum 30 mg per day, (j) no change
vous system (hereafter referred to as physiological) cue reactivity.
in treatment that could affect the desire to drink between the two cue exposure
The study used a placebo in both experimental conditions in order
sessions, (k) no hearing impairment, and (l) no anosmia or rhinitis. Participants
to avoid confounding the pharmacological effect of disulfiram
were not allowed to consume any alcohol during enrollment in the study. If drinkingoccurred, a delay of 6 days of abstinence was required before resuming participation.
with the psychological effect of the threat. We evaluated subjec-tive and physiological cue reactivity in relation to the threat of a
2.2. Design and procedure
We also tested possible associations between subjective and
The study was a crossover design, initially inspired by the cue reactivity assess-
physiological measures. Findings are contradictory with some stud-
ment developed by Monti and colleagues (Monti et al., 1987, 1993b; Rohsenow etal., 2000) and modified for the study objectives. Each participant was seen three
ies showing associations (Ludwig and Wikler, 1974; Ludwig et al.,
times. An inclusion visit occurred six or more days after consuming the last drink.
1977; Stormark et al., 1995), while others showed dissociations,
During this visit, the procedures and objectives of the experiment were explained
suggesting that during physiological cue reactivity (e.g., salivation)
and written informed consent obtained; the experimenter collected socio demo-
patients may not be aware of their urges (Monti et al., 1993a;
graphic data, administered the Mini International Psychiatric Interview (Sheehan et
Rohsenow and Monti, 1999; Reid et al., 2006). The independence of
al., 1998) for alcohol dependence, and collected data on alcohol consumption overthe past 6 months. Once written informed consent was obtained, participants com-
the two dimensions could influence how cue reactivity is evaluated
pleted the Alcohol Dependence Scale (ADS) (Skinner and Allen, 1982). The alcoholic
and interpreted.
drink that would most likely provoke a craving was selected by the participant who
Craving and aversion were evaluated on separate scales to
also described how it should be served. Patient identity was protected as per French
further understand their relationship to each other. Little evi-
law on biomedical research by unlinking the data file for analysis from all identifiers.
All procedures received institutional review board approval by the French board for
dence exists for their independence with alcohol dependent
protection of participants in biomedical research (CPP—Comité de protection des
patients contrary to other substance users where independence
personnes, Hôpital Pitié-Salpêtrière, Paris, France).
was demonstrated (Avants et al., 1995; Breiner et al., 1997; McEvoy
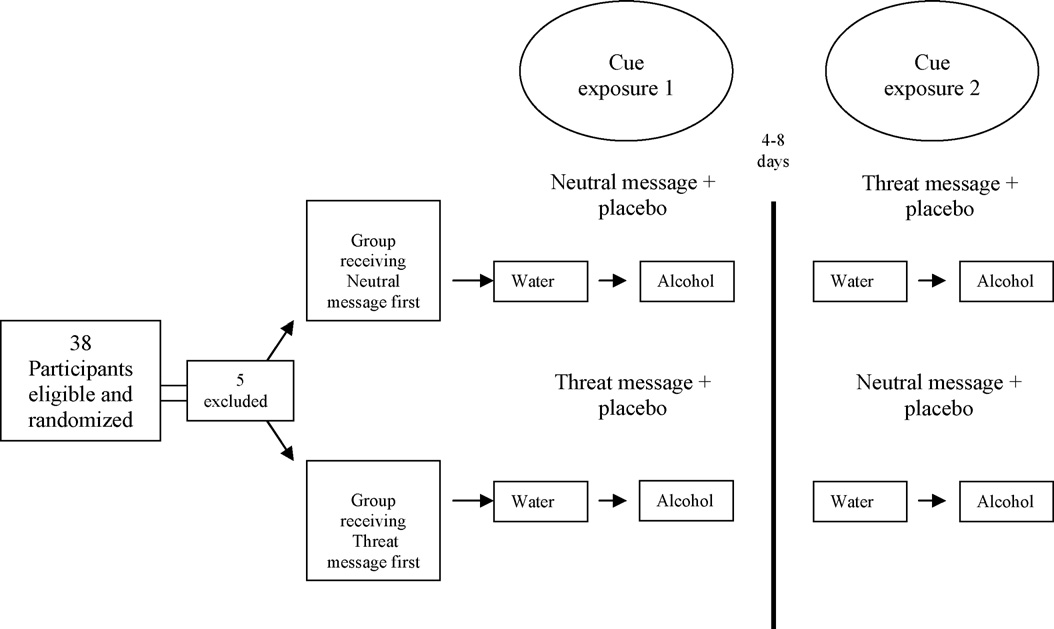
The two experimental beverage trials took place over the next 2 weeks (see
et al., 2004; Stritzke et al., 2004). This question is important for
Fig. 1). Each was associated with a neutral or threat message regarding the contents
future cue reactivity studies because if found independent, the two
of a placebo which was swallowed by the participants. The first trial occurred from 1to 7 days after the inclusion visit and the second after a wash out period of 4–8 days.
dimensions would best be evaluated on separate scales to avoid the
To counterbalance the message order, participants were randomized by blocks of 6
underreporting of the approach dimension. This is particularly rel-
into two groups. On the first beverage trial, half of the patients received a neutral
evant for patients who are ambivalent, that is both high in approach
message in French: This morning you have taken a tablet without any effect on a possible
and avoidance inclinations.
consumption of alcohol. If you had a drink, the alcohol would have the usual effect. Onthe second beverage trial, the same group received a threat message: This morning
Also evaluated were measures of levels of dependence and
you have taken a tablet that would rapidly provoke a strong, unpleasant reaction if
positive and negative affect as possible modulators of responses.
you consumed any alcohol – nausea, vomiting, an intense feeling of heat, very rapid
Physiological cue reactivity measures seem to be related to levels
heartbeat. But this tablet will have no effect if you do not consume any alcohol. The
of alcohol dependence (Kaplan et al., 1985; McCusker and Brown,
remaining half received the same messages but in the reverse order.
1991; Monti et al., 1993a), while the relationship of desire to drink
Each message was accompanied by the ingestion of a tablet at 8:10 a.m. for each
beverage trial. In both the threat and neutral conditions, the participants received
and dependence levels is inconsistent (Kaplan et al., 1985; Dolinsky
an identical placebo. The aim was to test only the psychological threat and not the
et al., 1987; Corty et al., 1988; Zilberman et al., 2003). Regarding
pharmacological effect of disulfiram.
affect, studies have shown that negative affect has been associ-
Each participant reported to the assessment room at 1:30 p.m. on the experi-
ated with craving (McCusker and Brown, 1991; Rohsenow et al.,
mental day. The experimenter explained and demonstrated the procedure (∼30 mn),but afterwards remained hidden from view behind a one-way mirror during most
1992; Baker et al., 2004; Fox et al., 2007). This study extends
of the experiment. Talking was not allowed. Participants sat at a table adjacent to
the research into another domain by asking how the threat of
the mirror. The materials needed during the beverage trials were behind the mirror:
a disulfiram–ethanol reaction compared to a no threat condition
the Colin monitor model no. BX-10Ma (used to evaluate blood pressure and heart
Author's personal copy
M.D. Skinner et al. / Drug and Alcohol Dependence 112 (2010) 239–246
Fig. 1. Cue exposure procedure.
rate), the alcoholic beverage and its commercial container, drinking related items,
This analysis was performed using a Mann–Whitney test comparing differences in
bottled mineral water, glasses, tray, opaque cover, and a CD player. All instructions
change scores (alcohol minus water exposure scores) of craving now between both
were recorded and played step by step. The Colin monitor blood pressure cuff was
randomisation order groups. A correlation of 0.7 between 2 craving measures of
attached to the participant's non-dominant arm during the entire session, but only
the same subject during the same visit was assumed. Moreover, measures from the
turned on during the three relaxation periods and two beverage trials.
literature (Monti et al., 1993b) of mean ± SD craving scores of water exposure fol-
The steps involved in each beverage trial were: a 3 min relaxation period, a 3 min
lowed by alcohol exposure were 2.7 ± 2.8 and 5.6 ± 3.3, respectively. Thus, baseline
water exposure, a time for completing the questionnaires, a 3 min relaxation period,
change scores of craving between alcohol and water exposure were estimated at
a 3 min alcohol exposure, a time for completing the questionnaires, and a 3 min
2.9 ± 2.4. We also hypothesized that with the threat of an aversive reaction, change
relaxation period with debriefing after the final trial. The experimenter filled the
score would be reduced by half, being equal to 1.45, with the same standard devia-
glass half full with either water or alcohol in front of the patient and then remained
tion of 2.4, and that the correlation between 2 change scores of craving in the same
behind the one-way mirror for the remainder of the session. Participants were sig-
subject would be 0.5. Consequently, the differences in change scores were expected
nalled to smell the drinks by 13 pairs of recorded high and low tones per 3 min
to be −1.45 ± 2.4 for the off-on (neutral-threat) sequence group and 1.45 ± 2.4 for
trial. The interval between the pairs was varied to prevent temporal conditioning.
the on-off (threat-neutral) sequence group. With alpha risk of 0.05 and beta risk
Instructions were given to hold the drink from 2 to 5 cm from the mouth and to
of 0.2, 28 patients were necessary for a non-parametric test. In order to take into
not drink the contents. The questionnaires referred to the desire for alcohol, even
account losses during the study, 38 patients were included.
during the water trial. As a reminder, the message given the morning of the trial wasrepeated immediately before each alcohol trial. At the end of the session, the partic-
2.4.2. Data analysis. The effects of alcohol exposure, threat, period, and interactions
ipant remained with the experimenter until there was no further desire for alcohol.
on cue reactivity measures were analyzed using multivariate linear modelling. The
At the end of the final session, the experimenter asked the participants about how
triple interaction alcohol-threat-period was tested as well as the carryover effect.
they perceived the experiment, possible coping strategies, and the experiment's
There was no significant alcohol by threat by period interaction and at a 10% signifi-
effect on their confidence level. At the conclusion of the experiment, participants
cance level, no carryover effect was found; the analyses were pursued to determine
were informed by letter of the results of the study and that they had received a
the effects of the threat and alcohol exposure on cue reactivity. The crossover design
placebo in both conditions.
allowed each parameter estimate derived from the model to be analyzed using theMann-Whitney test which was used to compare both randomisation order groups
2.3. Cue reactivity measures
(neutral followed by threat condition and threat followed by neutral condition). Atest of carryover effect was thus performed by calculating the sums of the change
2.3.1. Arterial blood pressure and heart rate. The Colin monitor, set to continuous
scores (alcohol exposure scores minus water exposure scores) for each participant
mode, collected and calculated mean heart rate and arterial blood pressure every
and then comparing the two randomisation order groups. The comparison of dif-
30 s during relaxation periods and during beverage trials. The results were stocked
ferences between second and first cue exposure visits for the change scores in each
in the Colin's microprocessor and printed based on each 15 s sampling period.
measure allowed for an analysis of the threat by alcohol exposure interaction. Like-wise, the comparison of differences between second and first cue exposure visits
2.3.2. Subjective measures. Immediately after each beverage trial, the participant
of the sum of water and alcohol exposure scores for each variable allowed for
filled out questionnaires consisting of five visual analogue scales of 100 mm long:
an analysis of the threat effect. Computational details are given in Supplementary
(1) How much do you want a drink right now? (craving now) (2) How much does
material available online and were based on the theory of non-parametric compar-
the idea of drinking turn you off right now? (aversion now) (3) If you were not at the
ison tests for a crossover design (Hills and Armitage, 1979).1 Unlike cue reactivity
hospital but rather in a situation where you habitually drank in the past, how much
measures, heart rate, systolic, and diastolic blood pressure were analyzed using
would you want a drink right now? (craving imaginary) (4) If you were not at the
a repeated measures ANOVA since these data were assumed to be normally
hospital but rather in a situation where you habitually drank in the past, how much
would the idea of drinking turn you off right now? (aversion imaginary) (5) Are you
Secondary analyses consisted of correlations between cue reactivity measures,
nauseated now? (nausea).
alcohol dependence scores, and affect and were analyzed using Spearman's rank
After completing the above questionnaire, the participant filled out the PANAS
order tests. These analyses were stratified according to threat and neutral condi-
(Positive and Negative Affect Scale) (Watson et al., 1988), an evaluation of affect
tions and adjusted for the period using a partial correlation coefficient. Data were
from the moment the beverage was poured into the glass.
described as means (SD) if the distribution was normal or by median (range) if not
Primary outcome measures were the change scores of cue reactivity during
normal. According to the definition of Baron and Kenny (1986), a moderator analysis
alcohol and water exposures between the threat and neutral conditions.
was performed testing the interaction effect between the moderator (PANAS) and
2.4. Statistical analyses
2.4.1. Calculation of the sample size. The main analysis consisted of calculating inter-
1 Additional materials are available with the online version of this article at
action exposure by condition effects on subjective cue reactivity (craving now).
Author's personal copy
M.D. Skinner et al. / Drug and Alcohol Dependence 112 (2010) 239–246
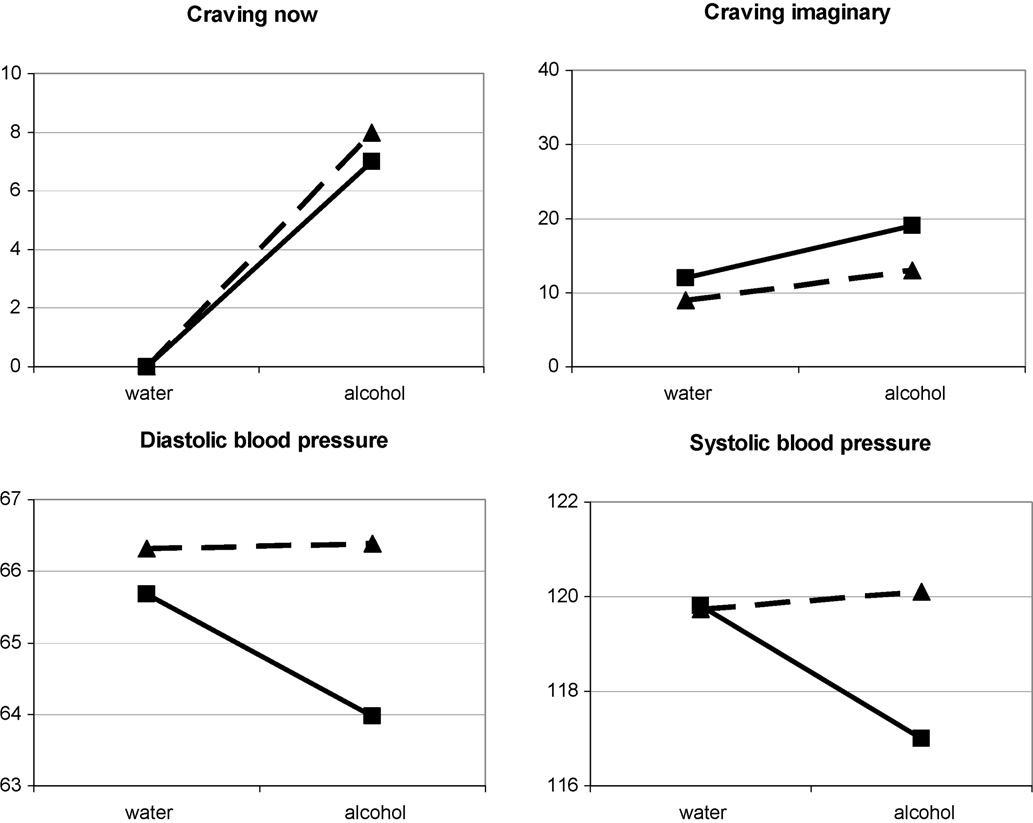
nificant condition by alcohol interaction for craving now, craving
Demographics, drinking history, and alcohol dependence score (ADS).
imaginary (see Table 2 and Fig. 3), or the PANAS.
3.4. Secondary analyses
Age, mean (SD), years
A period effect on cue reactivity was found for the scales crav-
ing now, (p = 0.039), craving imaginary (p = 0.048), diastolic blood
pressure (p = 0.002), and systolic blood pressure (p = 0.007). All
Married or cohabiting, no. (%)
decreased during the second exposure compared to the first. There
Unemployed, no. (%)
was no condition by alcohol interaction for the scale nausea. There
High school or greater, no. (%)
was no correlation between subjective and physiological measures.
Drinking historyAbstinence days over the past 6 months, median (range)
Regarding the relationship between desire (craving now) and aver-
Average weekly consumption g, median (range)
sion (aversion now), in both the neutral and threat conditions, there
ADS, median (range)
was a significant and inverse correlation (Spearman's � = −0.42,p = 0.02 and Spearman's = −0.39, p = 0.03, respectively). Alcoholdependence scores were not related to threat minus neutral change
the conditions (threat or neutral and water or alcohol) on cue reactivity measures in
scores (alcohol minus water scores) of the subjective measures
a mixed linear model. All statistical tests were two-tailed at a 5% significance level.
The analyses were performed using SAS/STAT software, Version 8.2 (SAS Institute,
for craving now, aversion now, and craving imaginary, nor for the
physiological measures. Dependence was, however, related to aver-sion imaginary, (Spearman's � = 0.43, p = 0.02). This result indicated
3. Results
that the more severely dependent participants were less turned offby drinking alcohol in an imaginary situation. Further exploration
3.1. Sample description
showed that this correlation occurred during the neutral condition(Spearman's � = −0.46, p = 0.01). When the threat was present, the
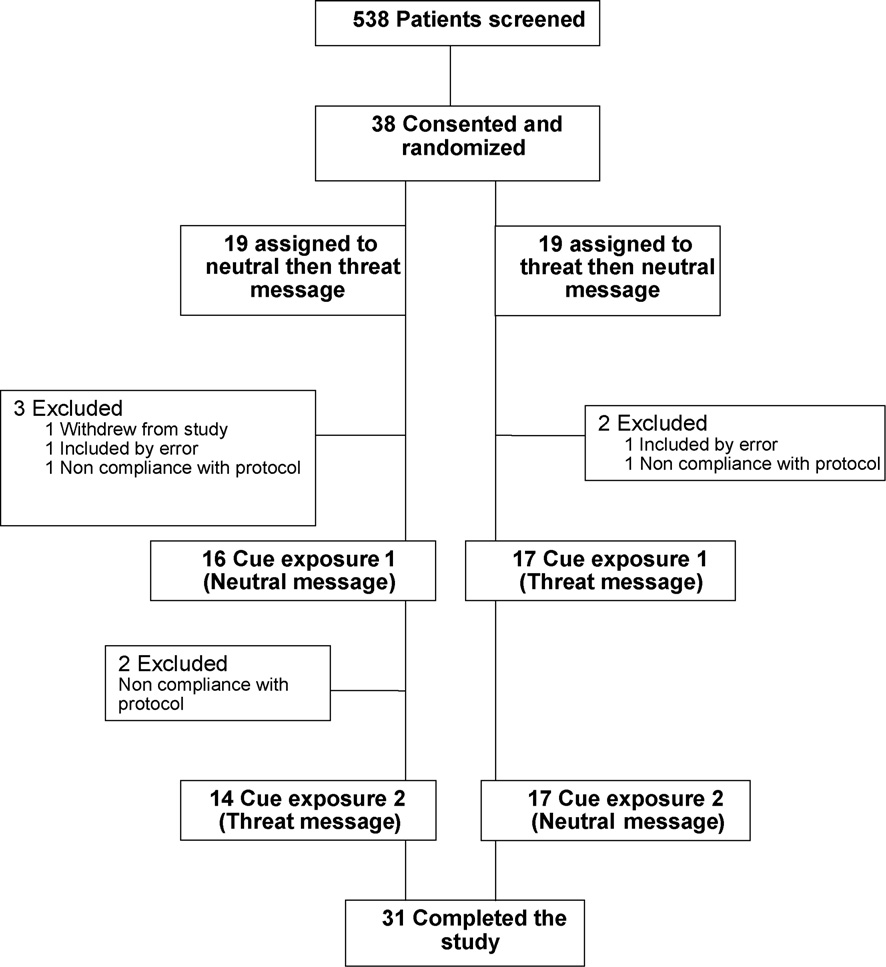
Of entering patients screened between November 2006 and
participants reacted the same way regardless of the level of depen-
September 2008 (n = 538), 38 were selected based on inclusion
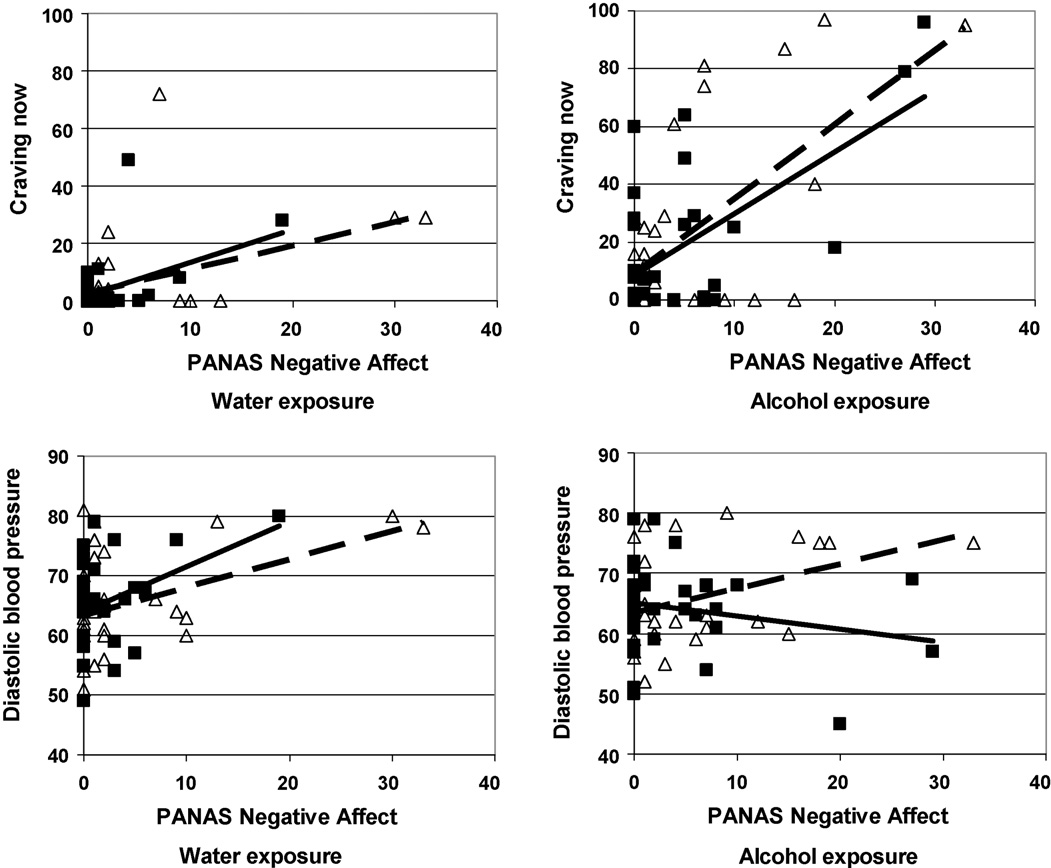
dence. PANAS negative affect increased during the alcohol exposure
criteria, provided consent, and were randomized to the order of
(p = 0.028) in both neutral and threat conditions (see Fig. 4).
threat and neutral conditions. Of these, 33 were analyzed. Demo-graphic and clinical characteristics are presented in Table 1. Five
3.5. Moderator analysis
participants were excluded. The exclusions occurred regardless ofthe randomisation order (see Fig. 2). Two patients did not partic-
Because PANAS negative affect was correlated with alcohol
ipate in the second beverage trial. After the first beverage trial,
exposure, we tested the hypothesis that negative affect moderated
one consumed alcohol and the other ingested acamprosate. We
the effect of a threat on alcohol cue reactivity (craving now). Inclu-
obtained and analyzed data only from the first exposure for these
sion of PANAS negative affect as a covariate in the condition by
two patients, bringing the total of completed studies to 31.
alcohol interaction model reduced the model's p-value from 0.41(NS) to 0.1. The relationship between negative affect and craving
3.2. Effect of alcohol on cue reactivity
was stronger during the threat condition or during alcohol expo-sure (in threat and neutral conditions) than during water exposure
The alcohol cue significantly increased the scales craving now.
in the neutral condition, which resulted in a significant triple inter-
(p < 0.0001), craving imaginary (p = 0.0027) and PANAS negative
action effect (PANAS negative affect by cue exposure by condition;
affect scores (p = 0.028). It had no effect on the other variables.
F = 6.08, p = 0.0034) on craving now (see Fig. 4).
We also tested the hypothesis that PANAS negative affect mod-
3.3. Effect of the threat condition on cue reactivity
erated the effect of a threat on diastolic blood pressure. The linearmixed model showed that diastolic blood pressure in response to
There was a significant condition by alcohol interaction on dias-
cue exposure or threat was modulated by PANAS negative affect
tolic blood pressure (p = 0.044) such that it decreased in response to
(triple interaction negative affect by cue exposure by condition;
the alcohol cue in the threat condition and remained the same in the
F = 11.94, p < 0.0001) (see Fig. 4).
neutral condition. The interaction term showed a trend (p = 0.071)
Because there was no effect of alcohol dependence (ADS) on
for systolic blood pressure. No condition by alcohol interaction
craving now, craving imaginary, and the physiological variables, its
occurred for the other measures, specifically, there was no sig-
moderator effect was not tested.
Table 2
Cue exposure responses in the neutral and threat conditions.
Neutral then threat message
Threat then neutral message
−0.5 (−46 to 48)
−2 (−73 to 56)
Craving imaginaryb
10.5 (−20 to 84)
Aversion imaginaryb
Heart rate (beats/min)c
Diastolic blood pressure (mm Hg)c
Systolic blood pressure (mm Hg)c
a Change scores consist of the difference between the alcohol exposure score and the water exposure score.
b Numbers are medians and (range).
c Numbers are means and (SD).
Author's personal copy
M.D. Skinner et al. / Drug and Alcohol Dependence 112 (2010) 239–246
Fig. 2. Flow chart of participant recruitment and retention.
were the most consistent and valid measures of cue reactivity(Rohsenow et al., 1990; Monti et al., 1999). This could be because
The primary purpose of this study was to determine whether
physiological measures are less likely to be under volitional con-
there was a difference in cue reactivity responses during a threat
trol (Reid et al., 2006) and are not dependent upon self-report.
condition compared to a neutral condition during alcohol cue expo-
In addition, several studies have shown that a physiological mea-
sure. First we established that our participants responded with
sure (salivation) predicted more drinking at follow up compared
increased desire to the alcohol cue. This was accompanied by an
to urge (Rohsenow et al., 1989, 1994). Few studies evaluated blood
increase in negative affect. Then we tested the effect of the threat
pressure, however, compared to heart rate, salivation and temper-
of a disulfiram–ethanol reaction condition compared to a neutral
ature (Niaura et al., 1988). In one study, blood pressure decreased in
condition on cue reactivity. To summarize our findings, no effect of
response to cues interpreted as an orienting, attentional response
a threat was found on craving. Regarding autonomic nervous sys-
to alcohol cues (Monti et al., 1999). It is possible that the decrease in
tem measures, we observed a decrease in diastolic blood pressure
blood pressure in the present study was associated with increased
during the threat compared to the neutral condition. Systolic blood
attention during the threat condition as the threat was repeated
pressure showed a trend, while heart rate remained unchanged.
just before the alcohol cue exposure, drawing the participant's
Inclusion of negative affect in the model strengthened the rela-
attention to the consequences of a possible consumption. Future
tionship between alcohol cue exposure and craving for alcohol and
studies specifically evaluating attention would be necessary to con-
decreased the diastolic blood pressure in response to cue exposure
firm this. A blood pressure decrease, which signifies a decrease in
in the threat condition. The threat of an aversive reaction during
sympathetic cardiovascular arousal (Critchley, 2005), could also
alcohol exposure was not associated with an increase in negative
arise from a reduced need for cognitive effort and any accompa-
affect, probably because temptation and risk were reduced, which
nying anxiety because the participants had less difficulty resisting
is reflected in the decrease in blood pressure.
temptation because of the support of believing they had ingested
Petrakis et al. (2005) have shown that alcohol dependent outpa-
tients treated with disulfiram had fewer anxiety related symptoms
Regarding secondary hypotheses, as we expected, subjective
compared to those treated with naltrexone or placebo. In addition,
and physiological responses varied independently. A similar dis-
it is probable that taking disulfiram facilitated a sense of control to
sociation was found by other investigators (Ooteman et al., 2006;
abstain from alcohol as suggested by an efficacy study of disulfiram
Carter and Tiffany, 1999; Niaura et al., 1988). Salivation was not
and acamprosate (Besson et al., 1998).
associated with urge (Cooney et al., 1984; Rohsenow et al., 1990;
Some authors who have measured both subjective and physio-
Monti et al., 1993b). The dissociation is not surprising if we con-
logical measures have suggested that heart rate and blood pressure
sider physiological processes to be multidetermined. Physiological
Author's personal copy
M.D. Skinner et al. / Drug and Alcohol Dependence 112 (2010) 239–246
Fig. 3. Variations of craving now (median), craving imaginary (median), diastolic blood pressure (mean), and systolic blood pressure (mean) by threat vs. neutral conditions
when exposed to water or alcohol. Continuous lines with square points represent the threat condition. Dotted lines with triangular points represent the neutral condition.
Fig. 4. Relationships between negative affect (PANAS), craving now, and diastolic blood pressure by exposure and threat vs. neutral conditions. Lines represent linear
regressions. Squares and continuous lines represent the threat condition. Triangles and dotted lines represent the neutral condition.
Author's personal copy
M.D. Skinner et al. / Drug and Alcohol Dependence 112 (2010) 239–246
processes are probably engaged in many functions unrelated to the
Further research is necessary to understand the relationship
cue manipulation (Rohsenow et al., 1990; Carter and Tiffany, 1999).
between disulfiram and the physiological as well as the psycho-
Patients were found unaware of their urges while salivating (Monti
logical responses to cues. Many questions remain unanswered
et al., 1993b; Rohsenow and Monti, 1999) and unaware of their
regarding the effect of a potential disulfiram–ethanol reaction on
physiological reactions during cue exposure (Ooteman et al., 2006),
decision-making, self-control, self-efficacy, commitment, atten-
indicating that a substantial number of alcohol dependent patients
tion, affect, and cognitive dissonance.
are unable to detect bodily sensations of craving. These findings do
In summary, physiological measures continue to be of value
not support conditioning models in which the physiological mea-
precisely because they lie outside of conscious control, are salient,
sures as well as the subjective measures should correlate (Ludwig
and replicable. The effect of the threat condition on diastolic blood
and Wikler, 1974; Baker et al., 1986).
pressure may reflect a psychophysiological mechanism involving
Contrary to our hypothesis, subjective craving and aversion
reductions in negative affect and increases in a sense of control,
were negatively correlated. As described in the multidimensional
attention, and commitment. Patients treated with disulfiram, if
ambivalence model (Breiner et al., 1999), craving and aversion were
they want to avoid a disulfiram–ethanol reaction, need to remind
thought to be two independent dimensions. Support for their inde-
themselves of the potential negative consequences that could arise
pendence has been shown (Avants et al., 1995; Breiner et al., 1997),
if they consume. The effort involved in being vigilant, despite crav-
but has yet to be validated among alcoholics. Because our partici-
ing, may divert them from their inclination to approach alcohol and
pants confirmed that they were committed to a goal of abstinence,
decrease negative affect. This could explain why disulfiram signifi-
they may have been less ambivalent, at least while hospitalized,
cantly reduces the number of drinking days with many patients. In
thus accounting for the correlation.
addition, it provides evidence to reframe disulfiram's image from
High levels of dependence have been shown to be associated
punitive to beneficial because of the relief it could provide from
with greater craving (Kaplan et al., 1985; Rohsenow et al., 1992;
the effortful, internal conflict inherent in deciding whether or not to
Monti et al., 1993b; Rohsenow and Monti, 1999; Drummond and
drink. This could help reverse the problem of treatment compliance,
Phillips, 2002). Our participants did not report a difference in crav-
the principle obstacle to the success of disulfiram.
ing according to the severity of dependence perhaps because ofsocial desirability bias. On the other hand, more severely dependent
Role of funding source
patients were not turned off by the idea of alcohol in an imaginarysituation as long as there was no threat. In the threat condition,
This study was supported by a grant from the Department of
however, they reacted in the same way as the less dependent.
Clinical Research and Development, Assistance Publique-Hôpitaux
Disulfiram treatment might thus be targeted to the most severely
de Paris (CIRC 05131), who provided clinical research assistance,
dependent patients to increase the aversion. There was no rela-
assistance with the statistical analyses, administrative support,
tionship between dependence and the physiological cue reactivity
methodological support, and placebo handling, but had no further
role in the writing of the report or in the decision to submit the
Several studies have shown negative affect to be associated
paper for publication. Funding was also provided by the Institut de
with craving although not specifically measured by the PANAS
Recherches Scientifiques sur les Boissons (IREB-Institute of Scien-
(McCusker and Brown, 1991; Rohsenow et al., 1992; Baker et al.,
tific Research on Drinks), who had no further role in the collection,
2004; Fox et al., 2007). This study was no exception. In the threat
analysis, and interpretation of the data; in the writing of the report;
condition or during alcohol exposure (in threat or neutral condi-
or in the decision to submit the paper for publication.
tions), the relationship between negative affect and craving nowwas stronger than in the neutral condition during water exposure,
indicating that negative affect modulated subjective craving.
Physiologically, as expected, participants with higher negative
Authors Skinner, Aubin, and Berlin designed the study and Skin-
affect also had higher blood pressure. An interaction was found
ner and Aubin wrote the protocol. Author Skinner managed the
between diastolic blood pressure, threat, exposure, and negative
literature searches, summaries of previous related work, and wrote
affect. The linear relationship between negative affect and diastolic
the first draft of the manuscript. Authors Coudert and Berlin under-
blood pressure was stronger in all of the conditions and exposures
took the statistical analyses. Author Passeri assisted in the data
except during the alcohol exposure in the threat condition. Even
collection and methodology of the protocol. Author Michel pro-
though negative affect prevailed for those participants who thought
vided clinical research assistance. All authors contributed to and
they had taken disulfiram, blood pressure was not affected. Perhaps
have approved the final manuscript.
those participants were less perturbed and had a stronger sense ofcontrol over alcohol intake than in the neutral condition where they
Conflict of interest
were less stable.
The present study has several limitations that need to be taken
Dr. Berlin is an employee of Université P. and M. Curie and Assis-
into consideration. One limit is that physiological cue reactivity is
tance Publique-Hôpitaux de Paris and reported having received
commonly viewed as multidetermined, that is, it could be activated
consulting fees from Pfizer Ltd. and Sanofi-Aventis. Dr. Aubin
by a number of different factors such as appetitive or aversive reac-
has received sponsorship to attend scientific meetings, speaker
tions (Glautier, 1999). Misinterpretation is possible, although it is
honorariums, and consultancy fees from Pfizer, McNeil, Glaxo-
reduced when the research questions are specific and the context
SmithKline, Pierre-Fabre Sante, Sanofi-Aventis, and Merck-Lipha.
well defined as in the present study. We might have included more
All other authors declare that they have no conflicts of interest.
various types of physiological measures that are less difficult tointerpret than blood pressure such as skin conductance and sali-
vation. Finally, there is the possibility of social desirability bias byour participants in order to convince the researchers or themselves
We thank Damaris Rohsenow, PhD for providing method-
of their capacity to cope with a craving. They were also enrolled
ological expertise, Arnaud Keslick for clinical research assistance,
in group cognitive behavioral therapy for relapse prevention dur-
Myriem Carrier, MD and Julie Tequi-Lebras for administrative sup-
ing part of the study which may have altered their responses to
port, Alain Mallet, MD, PhD for methodological support, and Annick
Tibi for placebo handling.
Author's personal copy
M.D. Skinner et al. / Drug and Alcohol Dependence 112 (2010) 239–246
Appendix A. Supplementary data
Ludwig, A., Wikler, A., 1974. Craving" and relapse to drink. Quart. J. Stud. Alcohol 35,
McCusker, C.G., Brown, K., 1991. The cue-responsivity phenomenon in dependent
Supplementary data associated with this article can be found, in
drinkers: ‘personality' vulnerability and anxiety as intervening variables. Br. J.
the online version, at doi:10.1016/j.drugalcdep.2010.06.011.
Addict. 86, 905–912.
McEvoy, P.M., Stritzke, W.G., French, D.J., Lang, A.R., Ketterman, R., 2004. Comparison
of three models of alcohol craving in young adults: a cross-validation. Addiction
99, 482–497.
Monti, P.M., Binkoff, J.A., Abrams, D.B., Zwick, W.R., Nirenberg, T.D., Liepman, M.R.,
American Psychiatric Association, 1994. Diagnostic and Statistical Manual of Mental
1987. Reactivity of alcoholics and nonalcoholics to drinking cues. J. Abnorm.
Disorders. American Psychiatric Association, Washington, DC.
Psychol. 96, 122–126.
Anton, R., Moak, D., Latham, P., 1995. The obsessive compulsive drinking scale
Monti, P.M., Rohsenow, D.J., Abrams, D.B., Zwick, W.R., Binkoff, J.A., Munroe,
(OCDS): a new method of assessing outcome in alcoholism treatment studies.
S.M., Fingeret, A.L., Nirenberg, T.D., Liepman, M.R., Pedraza, M., Kad-
Arch. Gen. Psychiatry 53, 225–231.
den, R.M., Cooney, N.L., 1993a. Development of a behavior analytically
Avants, S., Margolin, A., Kosten, T., Cooney, N., 1995. Differences between responders
derived alcohol-specific role-play assessment instrument. J. Stud. Alcohol 54,
and nonresponders to cocaine cues in the laboratory. Addict. Behav. 20, 215–224.
Baker, T., Morse, E., Sherman, J., 1986. The motivation to use drugs: a psychobiolog-
Monti, P.M., Rohsenow, D.J., Hutchison, K.E., Swift, R.M., Mueller, T.I., Colby, S.M.,
ical analysis of urges. Nebr. Symp. Motiv. 34, 257–323.
Brown, R.A., Gulliver, S.B., Gordon, A., Abrams, D.B., 1999. Naltrexone's effect on
Baker, T., Piper, M., McCarthy, D., Majeskie, M., Fiore, M., 2004. Addiction motivation
cue-elicited craving among alcoholics in treatment. Alcohol Clin. Exp. Res. 23,
reformulated: an affective processing model of negative reinforcement. Psychol.
Rev. 111, 33–51.
Monti, P.M., Rohsenow, D.J., Rubonis, A.V., Niaura, R.S., Sirota, A.D., Colby, S.M.,
Baron, R.M., Kenny, D.A., 1986. The moderator–mediator variable distinction in
Abrams, D.B., 1993b. Alcohol cue reactivity: effects of detoxification and
social psychological research: conceptual, strategic, and statistical considera-
extended exposure. J. Stud. Alcohol 54, 235–245.
tions. J. Pers. Soc. Psychol. 51, 1173–1182.
Mutschler, J., Grosshans, M., Koopmann, A., Hermann, D., Diehl, A., Mann, K., Kiefer, F.,
Besson, J., Aeby, F., Kasas, A., Lehert, P., Potgieter, A., 1998. Combined efficacy of
2010. Supervised disulfiram in relapse prevention in alcohol-dependent patients
acamprosate and disulfiram in the treatment of alcoholism: a controlled study.
suffering from comorbid borderline personality disorder—a case series. Alcohol
Alcohol Clin. Exp. Res. 22, 573–579.
Alcohol. 45, 146–150.
Breiner, M., Stritzke, W., Curtin, J., Patrick, C., Lang, A., 1997. Individuals respond
Niaura, R.S., Rohsenow, D.J., Binkoff, J.A., Monti, P.M., Pedraza, M., Abrams, D.B., 1988.
to appetitive cues based on learning histories with substances. In: American
Relevance of cue reactivity to understanding alcohol and smoking relapse. J.
Psychological, Society Meeting, Washington, DC.
Abnorm. Psychol. 97, 133–152.
Breiner, M., Stritzke, W., Lang, A., 1999. Approaching avoidance: a step essential to
Ooteman, W., Koeter, M.W., Verheul, R., Schippers, G.M., van den Brink, W., 2006.
the understanding of craving. Alcohol Res. Health 23, 197–206.
Measuring craving: an attempt to connect subjective craving with cue reactivity.
Carter, B.L., Tiffany, S.T., 1999. Meta-analysis of cue-reactivity in addiction research.
Alcohol Clin. Exp. Res. 30, 57–69.
Addiction 94, 327–340.
Petrakis, I.L., Poling, J., Levinson, C., Nich, C., Carroll, K., Rounsaville, B., 2005. Nal-
Chick, J., Gough, K., Falkowski, W., Kershaw, P., Hore, B., Mehta, B., Ritson, B., Ropner,
trexone and disulfiram in patients with alcohol dependence and comorbid
R., Torley, D., 1992. Disulfiram treatment of alcoholism. Br. J. Psychiatry 161,
psychiatric disorders. Biol. Psychiatry 57, 1128–1137.
Reid, M.S., Flammino, F., Starosta, A., Palamar, J., Franck, J., 2006. Physiological and
Cooney, N.L., Baker, L.H., Pomerleau, O.F., Josephy, B., 1984. Salivation to drinking
subjective responding to alcohol cue exposure in alcoholics and control subjects:
cues in alcohol abusers: toward the validation of a physiological measure of
evidence for appetitive responding. J. Neural Transm. 113, 1519–1535.
craving. Addict. Behav. 9, 91–94.
Robinson, T.E., Berridge, K.C., 2008. Review. The incentive sensitization theory of
Corty, E., O'Brien, C.P., Mann, S., 1988. Reactivity to alcohol stimuli in alcoholics: is
addiction: some current issues. Philos. Trans. R. Soc. Lond. B: Biol. Sci. 363,
there a role for temptation? Drug Alcohol Depend 21, 29–36.
Critchley, H.D., 2005. Neural mechanisms of autonomic, affective, and cognitive
Rohsenow, D., Monti, P., Abrams, D., Rubonis, A., Niaura, R., Sirota, A., Colby, S., 1992.
integration. J. Comp. Neurol. 493, 154–166.
Cue-elicited urges to drink and salivation in alcoholics: relationship to individual
De Sousa, A., 2004. A one-year pragmatic trial of naltrexone vs disulfiram in the
differences. Adv. Behav. Res. Therapy 14, 195–210.
treatment of alcohol dependence. Alcohol Alcohol. 39, 528–531.
Rohsenow, D.J., Monti, P.M., 1999. Does urge to drink predict relapse after treatment?
De Sousa, A., 2005. An open randomized study comparing disulfiram and acam-
Alcohol Res. Health 23, 225–232.
prosate in the treatment of alcohol dependence. Alcohol Alcohol. 40, 545–548.
Rohsenow, D.J., Monti, P.M., Hutchison, K.E., Swift, R.M., Colby, S.M., Kaplan, G.B.,
De Sousa, A.A., De Sousa, J., Kapoor, H., 2008. An open randomized trial compar-
2000. Naltrexone's effects on reactivity to alcohol cues among alcoholic men. J.
ing disulfiram and topiramate in the treatment of alcohol dependence. J. Subst.
Abnorm. Psychol. 109, 738–742.
Abuse Treat. 34, 460–463.
Rohsenow, D.J., Monti, P.M., Rubonis, A.V., Sirota, A.D., Niaura, R.S., Colby, S.M., Wun-
Diehl, A., Ulmer, L., Mutschler, J., Herre, H., Krumm, B., Croissant, B., Mann, K.,
schel, S.M., Abrams, D.B., 1994. Cue reactivity as a predictor of drinking among
Kiefer, F., 2010. Why is disulfiram superior to acamprosate in the routine clini-
male alcoholics. J. Consult. Clin. Psychol. 62, 620–626.
cal setting? A retrospective long-term study in 353 alcohol-dependent patients.
Rohsenow, D.J., Monti, P.M., Zwick, W.R., Nirenberg, T.D., Liepman, M.R., Binkoff,
Alcohol 45, 271–277.
J.A., Abrams, D.B., 1989. Irrational beliefs, urges to drink and drinking among
Dolinsky, Z.S., Morse, D.E., Kaplan, R.F., Meyer, R.E., Corry, D., Pomerleau, O.F., 1987.
alcoholics. J. Stud. Alcohol 50, 461–464.
Neuroendocrine, psychophysiological and subjective reactivity to an alcohol
Rohsenow, D.J., Niaura, R.S., Childress, A.R., Abrams, D.B., Monti, P.M., 1990. Cue
placebo in male alcoholic patients. Alcohol Clin. Exp. Res. 11, 296–300.
reactivity in addictive behaviors: theoretical and treatment implications. Int. J.
Drummond, D., Phillips, T.S., 2002. Alcohol urges in alcohol-dependent drinkers:
Addict. 25, 957–993.
further validation of the Alcohol Urge Questionnaire in an untreated community
Sheehan, D.V., Lecrubier, Y., Sheehan, K.H., Amorim, P., Janavs, J., Weiller, E., Her-
clinical population. Addiction 97, 1465–1472.
gueta, T., Baker, R., Dunbar, G.C., 1998. The mini-international neuropsychiatric
Fox, H.C., Bergquist, K.L., Hong, K.I., Sinha, R., 2007. Stress-induced and alcohol cue-
interview (M.I.N.I.): the development and validation of a structured diagnostic
induced craving in recently abstinent alcohol-dependent individuals. Alcohol
psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 59 (Suppl. 20),
Clin. Exp. Res. 31, 395–403.
22–33, quiz 34–57.
Fuller, R., Gordis, E., 2004. Does disulfiram have a role in alcoholism treatment today?
Skinner, H.A., Allen, B.A., 1982. Alcohol dependence syndrome: measurement and
Addiction 99, 21–24.
validation. J. Abnorm. Psychol. 91, 199–209.
Glautier, S., 1999. Do responses to drug-related cues index appetitive or aversive
Skinner, M.D., Aubin, H.J., 2010. Craving's place in addiction theory: contributions
states? Addiction 94, 346–347.
of the major models. Neurosci. Biobehav. Rev. 34, 606–623.
Hills, M., Armitage, P., 1979. The two-period cross-over clinical trial. Br. J. Clin.
Stormark, K.M., Laberg, J.C., Bjerland, T., Nordby, H., Hugdahl, K., 1995. Autonomic
Pharmacol. 8, 7–20.
cued reactivity in alcoholics: the effect of olfactory stimuli. Addict. Behav. 20,
Kaplan, R.F., Cooney, N.L., Baker, L.H., Gillespie, R.A., Meyer, R.E., Pomerleau, O.F.,
1985. Reactivity to alcohol-related cues: physiological and subjective responses
Stritzke, W.G., Breiner, M.J., Curtin, J.J., Lang, A.R., 2004. Assessment of substance
in alcoholics and nonproblem drinkers. J. Stud. Alcohol 46, 267–272.
cue reactivity: advances in reliability, specificity, and validity. Psychol. Addict.
Laaksonen, E., Koski-Jannes, A., Salaspuro, M., Ahtinen, H., Alho, H., 2008. A ran-
Behav. 18, 148–159.
domized, multicentre, open-label, comparative trial of disulfiram, naltrexone
Watson, D., Clark, L.A., Tellegen, A., 1988. Development and validation of brief mea-
and acamprosate in the treatment of alcohol dependence. Alcohol Alcohol 43,
sures of positive and negative affect: the PANAS scales. J. Pers. Soc. Psychol. 54,
Ludwig, A., Cain, R., Wikler, A., Taylor, R., Bendfeldt, F., 1977. Physiological and situa-
Zilberman, M.L., Tavares, H., el-Guebaly, N., 2003. Relationship between craving
tional determinants of drinking behavior. In: Gross, M. (Ed.), Alcohol Intoxication
and personality in treatment-seeking women with substance-related disorders.
and Withdrawal. Studies in Alcohol Dependence, Vol. B. Plenum Press, New York,
BMC Psychiatry 3, 1.
pp. 589–600.
Source: http://cesp-2016.vjf.inserm.fr/wp-content/uploads/productions/DAD3848.pdf
An evidence-based, Latin-American consensus ongastro-oesophageal reflux diseaseHenry Cohena, Joaquim Prado P. Moraes-Filhob, Maria Luisa Cafferatac,Giselle Tomassoc, Graciela Salisd, Oscar Gonza´leze, Jorge Valenzuelaf,Prateek Sharmag, Peter Malfertheinerh, David Armstrongi, Lars Lundellj,Rodolfo Cortik, Paulo Sakaib, Ivan Ceconellob and the Latin-AmericanGORD Consensus Group*
AIOS, CME SERIES (No. 23) Age Related Macular B. L. Sujata Rathod P. Manohar ALL INDIA OPHTHALMOLOGICAL SOCIETY This CME Material has been supported by the funds of the AIOS, but the views expressed therein do not reflect the official opinion of the AIOS. (As part of the AIOS CME Programme)