Levitra enthält Vardenafil, das eine kürzere Wirkdauer als Tadalafil hat, dafür aber schnell einsetzt. Männer, die diskret bestellen möchten, suchen häufig nach levitra kaufen ohne rezept. Dabei spielt die rechtliche Lage in der Schweiz eine wichtige Rolle.
Mlshb.gov.tw
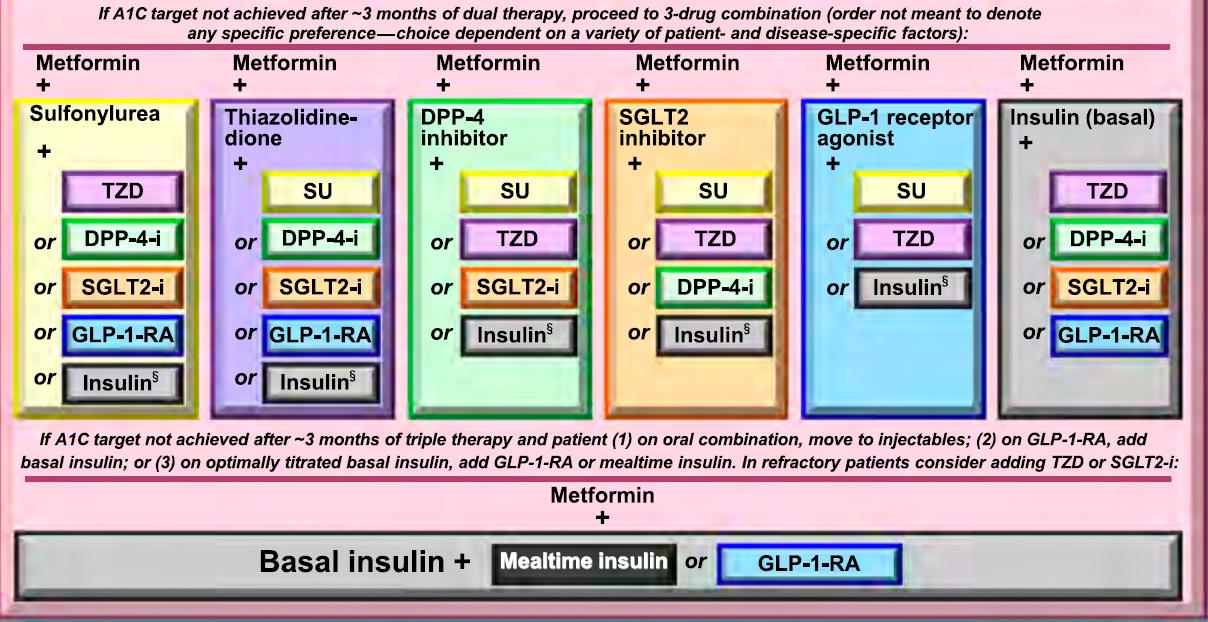
Strategies for Improving Care :
A patient-centered communication style that incorporates
patient preferences, assesses literacy and numeracy, and
addresses cultural barriers to care should be used. B
Treatment decisions should be timely and based on evidence-
based guidelines that are tailored to individual patient
preferences, prognoses, and comorbidities. B
Care should be aligned with components of the Chronic Care
Model to ensure productive interactions between a prepared
proactive practice team and an informed activated patient. A
When feasible, care systems should support team-based care,
community involvement, patient registries, and decision
support tools to meet patient needs. B
Diabetes Diagnosis
The patient 45 years old,
AC sugar : 120, PC sugar:170, A1C : 6.9
AC sugar : 130, PC sugar:170, A1C : 6.2
AC sugar : 110, PC sugar:230, A1C : 6.2
AC sugar : 110, OGTT PC sugar:230, A1C : 6.2
Confirming the Diagnosis for Diabetes
Unless there is a clear clinical diagnosis (e.g., patient in a
hyperglycemic crisis or with classic symptoms of hyperglycemia and
a random plasma glucose ≥200 mg/dL [11.1 mmol/L]), a second test
is required for confirmation.
It is recommended that the same test be repeated without delay
using a new blood sample for confirmation because there will be a
greater likelihood of concurrence.
If a patient has discordant results from two different tests, then the
test result that is above the diagnostic cut point should be
repeated. The diagnosis is made on the basis of the confirmed test.
For example, if a patient meets the diabetes criterion of the A1C
(two results ≥6.5% [48 mmol/mol]) but not FPG (<126 mg/dL [7.0
mmol/L]), that person should nevertheless be considered to have
Criteria for testing for diabetes or prediabetes in
asymptomatic adults
• Testing should be in all adults who
are overweight (BMI≧25 kg/m2
Obesity or≧23 kg/m2 in Asian Americans)
• Testing should begin at age 45
Testing for diabetes or prediabetes in asymptomatic adults
Physical inactivityFirst-degree relative with diabetesHigh-risk race/ethnicity (e.g., African American,
Latino, Native American, Asian American,Pacific
Women who delivered a baby weighing >9 lb or
were diagnosed with GDM
Hypertension (≧140/90 mmHg or on therapy for
Testing for diabetes or prediabetes in asymptomatic adults
HDL cholesterol level <35 mg/dL (0.90 mmol/L) and/or a
triglyceride level ≧250 mg/dL(2.82 mmol/L)
Women with polycystic ovary syndrome
A1C ≧5.7% (39 mmol/mol), IGT, or IFG on previous testing
Other clinical conditions associated with insulin resistance
(e.g., severe obesity, acanthosis nigricans)
History of CVD
Prevention or Delay of Type 2 Diabetes
Patients with prediabetes should be referred to an intensive diet and physical
activity behavioral counseling program adhering to the tenets of the Diabetes
Prevention Program (DPP) targeting a loss of 7% of body weight and should
increase their moderate-intensity physical activity (such as brisk walking) to at
least 150 min/week. A
Follow-up counseling and maintenance programs should be offered for long-
term success in preventing diabetes. B
Based on the cost-effectiveness of diabetes prevention, such programs should be
covered by third-party payers. B
Metformin therapy for prevention of type 2 diabetes should be considered in
those with prediabetes, especially in those with BMI >35 kg/m2, those aged <60
years, and women with prior gestational diabetes mellitus. A
Prevention or Delay of Type 2 Diabetes
At least annual monitoring for the development of diabetes in those with
prediabetes is suggested. E
Screening for and treatment of modifiable risk factors for cardiovascular disease is
suggested. B
Diabetes self-management education and support programs are appropriate
venues for people with prediabetes to receive education and support to develop
and maintain behaviors that can prevent or delay the onset of diabetes. B
Technology-assisted tools including Internet-based social
networks, distance learning, DVD-based content, and
mobile applications can be useful elements of effective
lifestyle modification to prevent diabetes. B

Obesity Management for the Treatment of Type 2
Diabetes : Recommendation
At each patient encounter, BMI should be calculated and documented in the
medical record. B
Diet, Physical Activity, and Behavioral Therapy :
Diet, physical activity, and behavioral therapy designed to achieve 5% weight loss
should be prescribed for overweight and obese patients with type 2 diabetes
ready to achieve weight loss. A
Such interventions should be high intensity (≥16 sessions in 6 months) and focus
on diet, physical activity, and behavioral strategies to achieve a 500–750 kcal/day
energy deficit. A
Diets that provide the same caloric restriction but differ in protein, carbohydrate,
and fat content are equally effective in achieving weight loss. A
Diet, Physical Activity, and Behavioral Therapy :
For patients who achieve short-term weight loss goals, long-term (≥1-year)
comprehensive weight maintenance programs should be prescribed. Such
programs should provide at least monthly contact and encourage ongoing
monitoring of body weight (weekly or more frequently), continued consumption
of a reduced calorie diet, and participation in high levels of physical activity (200–
300 min/week). A
To achieve weight loss of >5%, short-term (3-month) high-intensity lifestyle
interventions that use very low-calorie diets (≤800 kcal/day) and total meal
replacements may be prescribed for carefully selected patients by trained
practitioners in medical care settings with close medical monitoring. To maintain
weight loss, such programs must incorporate long-term comprehensive weight
maintenance counseling. B
Pharmacotherapy : Recommendations
When choosing glucose-lowering medications for overweight or obese patients
with type 2 diabetes, consider their effect on weight. E
Whenever possible, minimize the medications for comorbid conditions that are
associated with weight gain. E
Weight loss medications may be effective as adjuncts to diet, physical activity, and
behavioral counseling for selected patients with type 2 diabetes and BMI ≥27
kg/m2. Potential benefits must be weighed against the potential risks of the
If a patient's response to weight loss medications is <5% after 3 months or if there
are any safety or tolerability issues at any time, the medication should be
discontinued and alternative medications or treatment approaches should be
Bariatric Surgery : Recommendations
Bariatric surgery may be considered for adults with BMI >35 kg/m2 and type 2
diabetes, especially if diabetes or associated comorbidities are difficult to control
with lifestyle and pharmacological therapy. B
Patients with type 2 diabetes who have undergone bariatric surgery need lifelong
lifestyle support and annual medical monitoring, at a minimum. B
Although small trials have shown a glycemic benefit of bariatric surgery in patients
with type 2 diabetes and BMI 30–35 kg/m2, there is currently insufficient evidence
to generally recommend surgery in patients with BMI ≤35 kg/m2. E
Pharmacological Therapy for Type 1 Diabetes :
Most people with type 1 diabetes should be treated with multiple-dose insulin
injections (three to four injections per day of basal and prandial insulin) or
continuous subcutaneous insulin infusion. A
Consider educating individuals with type 1 diabetes on matching prandial insulin
dose to carbohydrate intake, premeal blood glucose, and anticipated activity. E
Most individuals with type 1 diabetes should use insulin analogs to reduce
hypoglycemia risk. A
Individuals who have been successfully using continuous subcutaneous insulin
infusion should have continued access after they turn 65 years of age. E
CARDIOVASCULAR DISEASE AND
"Atherosclerotic cardiovascular disease" (ASCVD) has replaced the former term "cardiovascular
disease" (CVD), as ASCVD is a more specific term.
Hypertension/Blood Pressure Control : Recommendations
Screening and Diagnosis
Blood pressure should be measured at every routine visit. Patients found to have
elevated blood pressure should have blood pressure confirmed on a separate
Goals
Systolic Targets
People with diabetes and hypertension should be treated to a systolic blood
pressure goal of <140 mmHg. A
Lower systolic targets, such as <130 mmHg, may be appropriate for certain
individuals with diabetes, such as younger patients, those with albuminuria,
and/or those with hypertension and one or more additional atherosclerotic
cardiovascular disease risk factors, if they can be achieved without undue
treatment burden. C
Hypertension/Blood Pressure Control : Recommendations
Diastolic Targets
Individuals with diabetes should be treated to a diastolic blood pressure goal of
<90 mmHg. A
Lower diastolic targets, such as <80 mmHg, may be appropriate for certain
individuals with diabetes, such as younger patients, those with albuminuria,
and/or those with hypertension and one or more additional atherosclerotic
cardiovascular disease risk factors, if they can be achieved without undue
treatment burden. B
Antiplatelet Agents : Recommendations
Consider aspirin therapy (75–162 mg/day) as a primary prevention strategy in
those with type 1 or type 2 diabetes who are at increased cardiovascular risk (10-
year risk >10%). This includes most men or women with diabetes aged ≥50 years
who have at least one additional major risk factor (family history of premature
atherosclerotic cardiovascular disease, hypertension, smoking, dyslipidemia, or
albuminuria) and are not at increased risk of bleeding. C
Aspirin should not be recommended for atherosclerotic cardiovascular disease
prevention for adults with diabetes at low atherosclerotic cardiovascular disease
risk (10-year atherosclerotic cardiovascular disease risk <5%), such as in men or
women with diabetes aged <50 years with no major additional atherosclerotic
cardiovascular disease risk factors, as the potential adverse effects from bleeding
likely offset the potential benefits. C
Antiplatelet Agents : Recommendations
In patients with diabetes <50 years of age with multiple other risk factors (e.g., 10-
year risk 5–10%), clinical judgment is required. E
Use aspirin therapy (75–162 mg/day) as a secondary prevention strategy in those
with diabetes and a history of atherosclerotic cardiovascular disease. A
For patients with atherosclerotic cardiovascular disease and documented aspirin
allergy, clopidogrel (75 mg/day) should be used. B
Dual antiplatelet therapy is reasonable for up to a year after an acute coronary
syndrome. B
DIABETIC KIDNEY DISEASE
"Nephropathy" was changed to "diabetic kidney disease" to emphasize that, while
nephropathy may stem from a variety of causes, attention is placed on kidney disease that is
directly related to diabetes.
Referral to a Nephrologist
Consider referral to a physician experienced in the care of kidney disease when
there is uncertainty about the etiology of kidney disease (absence of retinopathy,
heavy proteinuria, active urine sediment, or rapid decline in GFR).
Other triggers for referral may include difficult management issues (anemia,
secondary hyperparathyroidism, metabolic bone disease, resistant hypertension,
or electrolyte disturbances) or advanced kidney disease.
The threshold for referral may vary depending on the frequency with which a
provider encounters patients with diabetes and kidney disease. Consultation with
a nephrologist when stage 4 CKD develops (eGFR ≤30 mL/min/1.73 m2) has been
found to reduce cost, improve quality of care, and delay dialysis (). However,
other specialists and providers should also educate their patients about the
progressive nature of diabetic kidney disease, the kidney preservation benefits of
proactive treatment of blood pressure and blood glucose, and the potential need
for renal replacement therapy.
Diabetic Retinopathy
Antivascular Endothelial Growth Factor Treatment
While the ETDRS established the benefit of focal laser photocoagulation surgery
in eyes with clinically significant macular edema (defined as retinal edema located
at or within 500 μm of the center of the macula), current data from multiple well-
designed clinical trials demonstrate that intravitreal antivascular endothelial
growth factor (anti-VEGF) agents provide a more effective treatment regimen for
center-involved diabetic macular edema than monotherapy or even combination
therapy with laser.
Diabetic Retinopathy
Historically, laser photocoagulation surgery in both trials was beneficial in
reducing the risk of further visual loss in affected patients but generally not
beneficial in reversing already diminished acuity. Now, intravitreal therapy with
recombinant monoclonal neutralizing antibody to VEGF improves vision and has
replaced the need for laser photocoagulation in the vast majority of patients with
diabetic macular edema. Most patients require near-monthly administration of
intravitreal therapy with anti-VEGF agents during the first 12 months of treatment
with fewer injections needed in subsequent years to maintain remission from
center-involved diabetic macular edema. Other emerging therapies for
retinopathy that may use sustained intravitreal delivery of pharmacological agents
are currently under investigation.
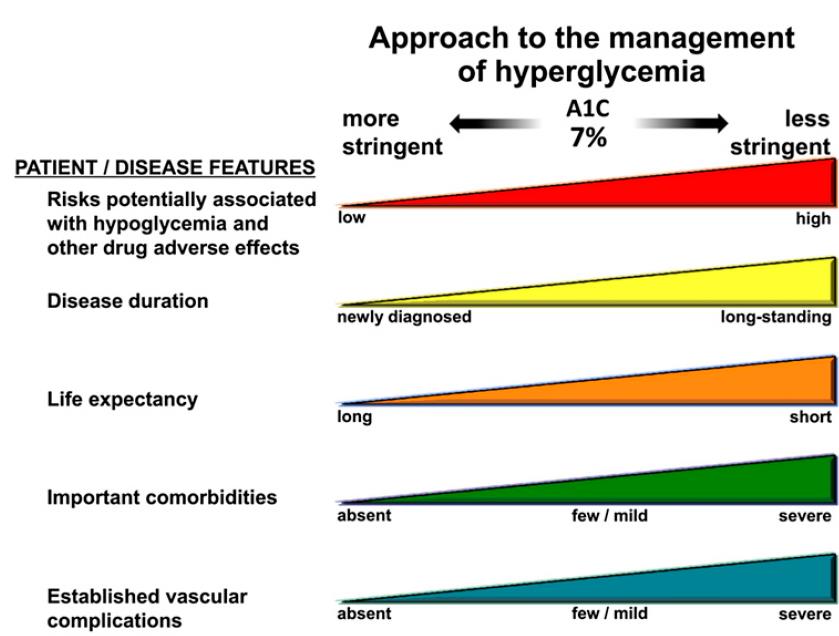
This represents a consensus framework for considering treatment goals for glycemia, blood pressure, and dyslipidemia in older adults with diabetes. The patient characteristic categories are general concepts. Not every patient will clearly fall into a particular category. Consideration of patient and caregiver preferences is an important aspect of treatment individualization. Additionally, a patient's health status and preferences may change over time. ADL, activities of daily living. ‡A lower A1C goal may be set for an individual if achievable without recurrent or severe hypoglycemia or undue treatment burden.
*Coexisting chronic illnesses are conditions serious enough to require medications or lifestyle management and may include arthritis, cancer, congestive heart failure, depression, emphysema, falls, hypertension, incontinence, stage 3 or worse chronic kidney disease, myocardial infarction, and stroke. By "multiple," we mean at least three, but many patients may have five or more
**The presence of a single end-stage chronic illness, such as stage 3–4 congestive heart failure or oxygen-dependent lung disease, chronic kidney disease requiring dialysis, or uncontrolled metastatic cancer, may cause significant symptoms or impairment of functional status and significantly reduce life expectancy.
†A1C of 8.5% (69mmol/mol) equates to an estimated average glucose of;200 mg/dL (11.1 mmol/L). Looser A1C targets above 8.5% (69mmol/mol) are not recommended as they may expose patients to more frequent higher glucose values and the acute risks from glycosuria, dehydration, hyperglycemic hyperosmolar syndrome, and poor wound healing.
CHILDREN AND ADOLESCENTS
Diabetes Self-management Education and Support :
Youth with type 1 diabetes and parents/caregivers (for patients aged <18 years)
should receive culturally sensitive and developmentally appropriate individualized
diabetes self-management education and support according to national
standards at diagnosis and routinely thereafter. B
Psychosocial Issues : Recommendations
At diagnosis and during routine follow-up care, assess psychosocial issues and
family stresses that could impact adherence to diabetes management and provide
appropriate referrals to trained mental health professionals, preferably
experienced in childhood diabetes. E
Encourage developmentally appropriate family involvement in diabetes
management tasks for children and adolescents, recognizing that premature
transfer of diabetes care to the child can result in nonadherence and deterioration
in glycemic control. B
Consider mental health professionals as integral members of the pediatric
diabetes multidisciplinary team. E
Glycemic Control : Recommendation
An A1C goal of <7.5% (58 mmol/mol) is recommended across all pediatric age-
groups. E
Autoimmune Conditions
Assess for the presence of additional autoimmune conditions soon after the
diagnosis and if symptoms develop. E
Thyroid Disease : Recommendations
Consider testing children with type 1 diabetes for antithyroid peroxidase and
antithyroglobulin antibodies soon after the diagnosis. E
Measure thyroid-stimulating hormone concentrations soon after the diagnosis of
type 1 diabetes and after glucose control has been established. If normal, consider
rechecking every 1–2 years or sooner if the patient develops symptoms
suggestive of thyroid dysfunction, thyromegaly, an abnormal growth rate, or an
unexplained glycemic variation. E
Hypertension : Recommendations
Blood pressure should be measured at each routine visit. Children found to have
high-normal blood pressure (systolic blood pressure or diastolic blood pressure ≥90th percentile for age, sex, and height) or hypertension (systolic blood pressure
or diastolic blood pressure ≥95th percentile for age, sex, and height) should have
blood pressure confirmed on 3 separate days. B
Initial treatment of high-normal blood pressure (systolic blood pressure or
diastolic blood pressure consistently ≥90th percentile for age, sex, and height)
includes dietary modification and increased exercise, if appropriate, aimed at
weight control. If target blood pressure is not reached with 3–6 months of
initiating lifestyle intervention, pharmacological treatment should be
In addition to lifestyle modification, pharmacological treatment of hypertension
(systolic blood pressure or diastolic blood pressure consistently ≥95th percentile
for age, sex, and height) should be considered as soon as hypertension is
confirmed. E
ACE inhibitors or angiotensin receptor blockers should be considered for the
initial pharmacological treatment of hypertension, following reproductive
counseling due to the potential teratogenic effects of both drug classes. E
The goal of treatment is blood pressure consistently <90th percentile for age, sex,
and height. E
Dyslipidemia : Recommendations
Testing
Obtain a fasting lipid profile in children ≥10 years of age soon after the diagnosis
(after glucose control has been established). E
If lipids are abnormal, annual monitoring is reasonable. If LDL cholesterol values
are within the accepted risk level (<100 mg/dL [2.6 mmol/L]), a lipid profile
repeated every 3–5 years is reasonable. E
Initial therapy should consist of optimizing glucose control and medical nutrition
therapy using a Step 2 American Heart Association diet to decrease the amount of
saturated fat in the diet. B
After the age of 10 years, addition of a statin is suggested in patients who, despite
medical nutrition therapy and lifestyle changes, continue to have LDL cholesterol
>160 mg/dL (4.1 mmol/L) or LDL cholesterol >130 mg/dL (3.4 mmol/L) and one or
more cardiovascular disease risk factors. E
The goal of therapy is an LDL cholesterol value <100 mg/dL (2.6 mmol/L). E
Diabetic Kidney Disease
Annual screening for albuminuria with a random spot urine sample for albumin–
to–creatinine ratio should be considered once the child has had diabetes for 5
Estimate glomerular filtration rate at initial evaluation and then based on age,
diabetes duration, and treatment. E
Treatment with an ACE inhibitor, titrated to normalization of albumin excretion,
should be considered when elevated urinary albumin–to–creatinine ratio (>30
mg/g) is documented with at least two of three urine samples. These should be
obtained over a 6-month interval following efforts to improve glycemic control
and normalize blood pressure.B
Consider an annual comprehensive foot exam for the child at the start of puberty
or at age ≥10 years, whichever is earlier, once the youth has had type 1 diabetes
for 5 years. E
Pregestational Diabetes : Recommendations
Provide preconception counseling that addresses the importance of glycemic
control as close to normal as is safely possible, ideally A1C <6.5% (48 mmol/mol),
to reduce the risk of congenital anomalies. B
Family planning should be discussed and effective contraception should be
prescribed and used until a woman is prepared and ready to become pregnant. A
Women with preexisting type 1 or type 2 diabetes who are planning pregnancy or
who have become pregnant should be counseled on the risk of development
and/or progression of diabetic retinopathy. Eye examinations should occur before
pregnancy or in the first trimester and then be monitored every trimester and for
1 year postpartum as indicated by degree of retinopathy. B
Gestational Diabetes Mellitus
Lifestyle change is an essential component of management of gestational
diabetes mellitus and may suffice for treatment for many women. Medications
should be added if needed to achieve glycemic targets. A
Preferred medications in gestational diabetes mellitus are insulin and metformin;
glyburide may be used but may have a higher rate of neonatal hypoglycemia and
macrosomia than insulin or metformin. Other agents have not been adequately
studied. Most oral agents cross the placenta, and all lack long-term safety data. A
General Principles for Management of Diabetes in
Potentially teratogenic medications (ACE inhibitors, statins, etc.) should be
avoided in sexually active women of childbearing age who are not using reliable
Fasting, preprandial, and postprandial self-monitoring of blood glucose are
recommended in both gestational diabetes mellitus and pregestational diabetes
in pregnancy to achieve glycemic control. B
Due to increased red blood cell turnover, A1C is lower in normal pregnancy than in
normal nonpregnant women. The A1C target in pregnancy is 6–6.5% (42–48
mmol/mol); <6% (42 mmol/mol) may be optimal if this can be achieved without
significant hypoglycemia, but the target may be relaxed to <7% (53 mmol/mol) if
necessary to prevent hypoglycemia. B
The American College of Obstetricians and Gynecologists (ACOG) (
recommends the following targets for women with pregestational type 1 or type 2
Fasting ≤90 mg/dL (5.0 mmol/L)
One-hour postprandial ≤130–140 mg/dL (7.2–7.8 mmol/L)
Two-hour postprandial ≤120 mg/dL (6.7 mmol/L)
After diagnosis, treatment starts with medical nutrition therapy, physical activity,
and weight management depending on pregestational weight, as outlined in the
section on pregestational type 2 diabetes below, and glucose monitoring aiming
for the targets recommended by the Fifth International Workshop-Conference on
Gestational Diabetes Mellitus ):
Fasting ≤95 mg/dL (5.3 mmol/L) and either
One-hour postprandial ≤140 mg/dL (7.8 mmol/L) or
Two-hour postprandial ≤120 mg/dL (6.7 mmol/L)
A major barrier to effective preconception care is the fact that the majority of
pregnancies are unplanned. Planning pregnancy is critical in women with
pregestational diabetes due to the need for preconception glycemic control and
preventive health services. Therefore, all women with diabetes of childbearing age
should have family planning options reviewed at regular intervals. This applies to
women in the immediate postpartum period. Women with diabetes have the
same contraception options and recommendations as those without diabetes.
The risk of an unplanned pregnancy outweighs the risk of any given contraception
Women with greater initial degrees of hyperglycemia may require early initiation
of pharmacological therapy. Treatment has been demonstrated to improve
perinatal outcomes in two large randomized studies as summarized in a U.S.
Preventive Services Task Force review . Insulin is the first-line agent recommended
for treatment of GDM in the U.S. Individual randomized controlled trials support
the efficacy and short-term safety of metformin (pregnancy category B) and
glyburide (pregnancy category B) for the treatment of GDM. However, both
agents cross the placenta, and long-term safety data are not available for either
Insulin
Insulin may be required to treat hyperglycemia, and its use should follow the
More recently, several meta-analyses and large observational studies examining
maternal and fetal outcomes have suggested that sulfonylureas, such as glyburide,
may be inferior to insulin and metformin due to increased risk of neonatal
hypoglycemia and macrosomia with this class.
Metformin, which is associated with a lower risk of hypoglycemia and potential
lower weight gain, may be preferable to insulin for maternal health if it suffices to
control hyperglycemia (however, metformin may slightly increase the risk
of prematurity. None of these studies or meta-analyses evaluated long-term
outcomes in the offspring. Thus, patients treated with oral agents should be
informed that they cross the placenta and, while no adverse effects on the fetus
have been demonstrated, long-term studies are lacking.
Perioperative Care Standards for perioperative care
Target glucose range for the perioperative period should be 80–180mg/dL (4.4–
Preoperative risk assessment for patients at high risk for ischemic heart disease
and those with autonomic neuropathy or renal failure.
The morning of surgery or procedure, hold any oral hypoglycemic agents and give
half of NPH dose or full doses of a long-acting analog or pump basal insulin.
Monitor blood glucose every 4–6 h while NPO and dose with shortacting
insulin as needed.
Diabetes Care in the Hospital
A basal plus bolus correction insulin regimen is the preferred treatment for
noncritically ill patients with poor oral intake or those who are taking nothing by
mouth. An insulin regimen with basal, nutritional, and correction components is
the preferred treatment for patients with good nutritional intake. A
The sole use of sliding scale insulin in the inpatient hospital setting is strongly
Insulin therapy should be initiated for treatment of persistent hyperglycemia
starting at a threshold ≧180 mg/dL (10.0 mmol/L). Once insulin therapy is started,
a target glucose range of 140–180 mg/dL (7.8–10.0 mmol/L) is recommended for
the majority of critically ill patients A and noncritically ill patients. C
Source: http://www.mlshb.gov.tw/upload/20/2016042614040152793.pdf
December 2010 OH&S FAST FACTS: Drugs that fight cancer and other hazardous agents are valuable and vital to the care of patients. Health care workers need to know the hazards they Your Health. Your Safety. are dealing with to ensure they remain safe while caring for their patients. Hazardous Drugs in Health Care Drugs that meet one or more of
Land West of Horsham Stakeholders Consultation Report November 2006 Table of Contents 1. Introduction 2. The Core Strategy 3. Masterplan 4. Transport Stakeholders Consultation 22nd November 5. Community & Leisure Stakeholders Consultation 30th Appendix 1. Event Horsham District Council