Levitra enthält Vardenafil, das eine kürzere Wirkdauer als Tadalafil hat, dafür aber schnell einsetzt. Männer, die diskret bestellen möchten, suchen häufig nach levitra kaufen ohne rezept. Dabei spielt die rechtliche Lage in der Schweiz eine wichtige Rolle.
Physiciansinstitute.org



and Treatment of
in Primary Care
This educational activity is supported through pooled-funded
educational grants from Pfizer Inc. and Abbott Laboratories to the
Physicians' Institute for Excellence in Medicine to develop and offer
grants to accredited CME providers for improvement in the diagnosis
and treatment of rheumatoid arthritis. The Physicians' Institute retains
full control over the distribution of individual grants under this program.
Estimated Time to Complete Activity: 1.5 hours
Publication Date: November 2010
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
Who shoulD PaRTiCiPaTE
This activity is designed for primary care clinicians
Kenneth G. Saag, MD, MSc
(family practice and general internal medicine), including
physicians, nurse practitioners, nurses, physician
Jane Knight Lowe Professor of Medicine,
assistants, and other members of the healthcare team
Division of Clinical Immunology and Rheumatology
involved in the diagnosis and treatment of patients with
Professor of Epidemiology,
rheumatoid arthritis (RA).
University of Alabama at Birmingham (UAB) School
of Public Health
Deep South Musculoskeletal Center for Education
Early diagnosis and treatment of RA are critical to optimal
and Research on Therapeutics
patient outcomes, yet delays in diagnosis are common
Associate Director, Multidisciplinary Clinical
given the many competing diagnoses and RA's variability
in presentation. This monograph will help primary care
Director, UAB Center for Outcomes and Effectiveness
clinicians develop practice-based strategies to overcome
Research and Education
challenges in the timely screening, diagnosis, and
treatment of their patients with RA. This brief primer aims
to clarify the keys to RA diagnosis, considerations when
Leonard M. Fromer, MD, FAAFP, Dipl. ABFM
initiating disease-modifying antirheumatic drug therapy,
Assistant Clinical Professor,
and confidence-building methods for discussing RA with
Department of Family Medicine
patients to promote ongoing dialogue and treatment
David Geffen School of Medicine
University of California, Los Angeles
Los Angeles, California
Assistant Clinical Professor,
At the conclusion of this activity, participants should be
Western University of Health Sciences
1. Distinguish the clinical signs, tests, and symptoms that
accompany RA as compared to other disorders.
2. Facilitate patient referral in a timely manner
Jacqueline W. Fincher, MD, FACP
to a specialist when necessary, and initiate
Managing Partner,
prompt treatment if a specialist appointment
McDuffie Medical Associates
is not readily available.
3. Utilize evidence-based clinical guidelines,
Governor-Elect, Georgia Chapter,
medical education, and quality improvement
American College of Physicians
to ensure appropriate initiation and/or monitoring
of treatment.
4. Implement preventive measures, such as screening
The faculty reported the following:
for comorbidities that may result from RA or
Kenneth G. Saag, MD, MSc
Consulting
Amgen, AstraZeneca,
5. Educate patients and caregivers about RA
Eli Lilly and Company, Genentech,
concerning the disease and treatments and
Horizon, sanofi-aventis, Merck,
the importance of compliance.
Novartis, and Pfizer Inc.
Speakers Bureau
Amgen, Eli Lilly and Company,
and Novartis
Leonard M. Fromer, MD, FAAFP, Dipl. ABFM
Dr. Fromer has disclosed that he has no actual or
potential conflict of interest in regard to this activity.
Jacqueline W. Fincher, MD, FACP
Dr. Fincher has disclosed that she has no actual or
potential conflict of interest in regard to this activity.
The audience is advised that this educational
Planning Staff
activity will not include reference(s) to unlabeled
The planning staff of the Physicians' Institute for
or unapproved uses of drugs or devices.
Excellence in Medicine and CME Enterprise have nothing
to disclose.
Disclaimer: The views and opinions expressed in this activity are those of the faculty and do not necessarily reflect the views of
the Physicians' Institute for Excellence in Medicine or CME Enterprise or recommendations of the sponsor or commercial supporters.
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
inflammation called synovitis that involves both small
and large joints and that, over time, can lead to
Musculoskeletal disorders and diseases (MSDs)
progressive joint destruction and loss of function. In the
are the leading cause of disability in the United
United States, nearly 1.3 million people have RA, affecting
States and account for more than one-half of all chronic
all races and ethnic groups and 2.5 times as many women
conditions in people over 50 years of age in developed
as men.4 From an economic standpoint, costs for the
countries. The economic impact of MSD is also
medical and surgical treatment for rheumatoid arthritis
staggering. In 2004, the sum of the direct expenditures
and the wages lost because of disability have been
in healthcare costs and the indirect expenditures in lost
estimated to be as high as $19 billion per year.5 Untreated,
wages was estimated to be $849 billion, or 7.7% of the
the majority of patients with RA become disabled, with
national gross domestic product.1
as many as 80% exhibiting a compromise in activities of
MSDs can be classified as arthritis, connective tissue
daily living after 10 to 20 years of disease. Fortunately,
diseases, soft tissue rheumatism, osteoporosis, and
appropriate application of disease-modifying therapy can
orthopedic injury. Arthritis, soft tissue rheumatism, and
reduce that potential for disability by more than 60%.6
osteoporosis constitute rheumatic diseases, characterized
by pain and inflammation in the joints and associated
structures, along with muscle soreness and stiffness.
ThE RolE oF ThE
PRimaRy CaRE PhysiCian
Arthritis is a common MSD that affects 46 million
Americans, or roughly 1 in 3 people in the United States.
The primary care physician (PCP) (or, in some cases, nurse
More than half of all people ages 65 and over have
practitioner or physician assistant) is generally the first
osteoarthritis (OA), the most common form of arthritis.
to see the patient who exhibits rheumatologic symptoms
More than two-thirds of people affected by arthritis
and thus can have the most critical effect on the patient's
are women.2
disease progression. If RA can be diagnosed and
aggressive treatment begun before radiologic symptoms
A leading cause of disability, arthritis is associated with
set in, a better outcome is possible. If diagnosis, referral,
more job loss and impairment than any other disease.
and treatment are delayed until the most prominent
Over $100 billion each year in medical costs and lost
clinical manifestations of the disease are present, the
wages is attributed to arthritis.3 It is estimated to
prognosis is not as good.7
account for 4.6% of all ambulatory care visits, about
36 million each year. And, as the population ages, the
Early symptom recognition, early pain management,
future burden is projected at 63 million people by the
provisional diagnosis, and timely referral to a
year 2025.4
rheumatologist or other specialist for early and
aggressive treatment strategies are critical to improving
Figure 1 lists prototypes for the different forms of
chances of remission (or achieving optimal patient
rheumatic disease and examples of medications that
outcomes when low disease activity or remission is not
might be used in treatment.
possible). Early initiation of disease-modifying therapies
can slow the progression of bone erosions, improving
all aspects of RA disease activity and enabling optimal
Categories
of Rheumatic Disease
physical function.8
n Example
The 2002 American College of Rheumatology (ACR)
Guidelines noted that
Cartilage d
". . the majority of the care of patients with RA may be
provided by a single physician (primary care
physician or rheumatologist who also provides primary
care) or the responsibility may be shared. The role
of the primary care physician is to recognize and
Tennis elbow
diagnose RA at its onset and to ensure that the patient
receives timely treatment before permanent joint
damage has occurred. The rheumatologist should
provide support and consultation to the patient and
Figure 1. Categories of Rheumatic Disease
his or her primary care physician in the diagnosis and
treatment of the RA. If the care of a patient with RA is
to be shared, an explicit plan for monitoring RA disease
RA is the most common form of inflammatory arthritis,
activity and/or drug toxicity needs to be formulated."9
a condition where arthritis is present because of
localized joint inflammation. In RA, it's the joint lining
that's involved. RA is characterized by symmetrical
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
Despite ACR guidelines that support early referral
ClassiFiCaTion CRiTERia
to a rheumatologist and timely initial treatment
FoR RhEumaToiD aRThRiTis
in order to prevent or slow disease progression
Classification criteria are not diagnostic criteria, but
and long-term disability,9,10 the referral rate to
they provide clinicians with a framework for evaluating
rheumatologists remains low.9,10 Guidelines recommend
the patient's clinical manifestations of disease and
that patients who fit clinical criteria for RA should
categorizing them as more or less indicative of RA since
be referred within 6 weeks of symptom onset when
there are no surefire diagnostic tests or radiographic
possible, but no later than within 3 months of consistent
findings that determine a definitive diagnosis. RA
symptoms, yet research shows that half of patients with
competes with a number of diseases with similar signs
RA are not referred within 6 months of disease onset,
and symptoms in the physician's mind, and the time
and therefore may not be receiving adequate early
taken to narrow down the field can mean increased
therapy.11 Patients frequently have RA symptoms for an
disease progression for the patient ultimately diagnosed
average of 9-12 months before a diagnosis is made, and
frequently wait additional months before a referral to a
rheumatologist is arranged.11
Table 1. Differential Diagnosis
of Rheumatoid Arthritis
Many primary care practitioners see few cases of RA
due to its relatively low prevalence, making it difficult
Connective tissue diseases such as scleroderma,
to gain experience with its diagnosis and management,
systemic lupus erythematosus, and psoriatic arthritis
thus precluding critical early specialist referral and
treatment. Diagnosing and treating RA requires a
team effort involving the patient and several levels of
healthcare professionals. Given the chronic and unstable
course of RA, an optimal longitudinal treatment plan
is necessary with comprehensive coordinated care
Juvenile rheumatoid arthritis
and the expertise of numerous healthcare providers,
Lyme disease
primarily the PCP and the rheumatologist. Essential
components of patient care management include
systematic and regular evaluation of disease activity,
patient education, rehabilitation interventions, use of
disease-modifying antirheumatic drugs (DMARDs) and
minimizing the impact of treatment on the individual's
function, assessment of treatment program adequacy,
and general health maintenance.9
Upon a provisional diagnosis, the PCP should assess
patient factors, such as likelihood of compliance and
Seronegative spondyloarthropathies,
comorbid diseases. Once the rheumatologist confirms
the provisional diagnosis, he or she provides a prognosis
and treatment plan as well as support and consultation
to the patient and the attending PCP. Even if the
disease has progressed, with referral and treatment and
subsequent screening for comorbidities and adverse
Recognizing that new treatment modalities make
events, radiographic progression can be attenuated and
early diagnosis of RA imperative, and that previous
the patient's quality of life improved.
classification criteria were too dependent on the signs
of disease no longer in its early stages, the ACR and
European League Against Rheumatism (EULAR) recently
updated classification criteria for RA. These updated
criteria provide a framework for the diagnosis of early
disease based on the unexplained presence of synovitis
in at least one joint along with an assessment of the
number and site of involved joints, serologic abnormality,
elevated acute phase response, and symptom duration.12
The new classification criteria also include the anti-cyclic
citrullinated peptide (anti-CCP) test as an alternate to
rheumatoid factor (RF) for establishing an RA diagnosis.
These criteria support a provisional diagnosis of RA
on the part of the PCP and immediate referral to a
rheumatologist for definitive diagnosis of RA or some
other rheumatic disease, as warranted.
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
The previous criteria, published in 1987, while useful in
joinT DisTRibuTion
differentiating RA from other inflammatory disorders, did
anD CliniCal FEaTuREs
not have the benefit of recent data indicating that RA
could be provisionally identified before the symptoms of
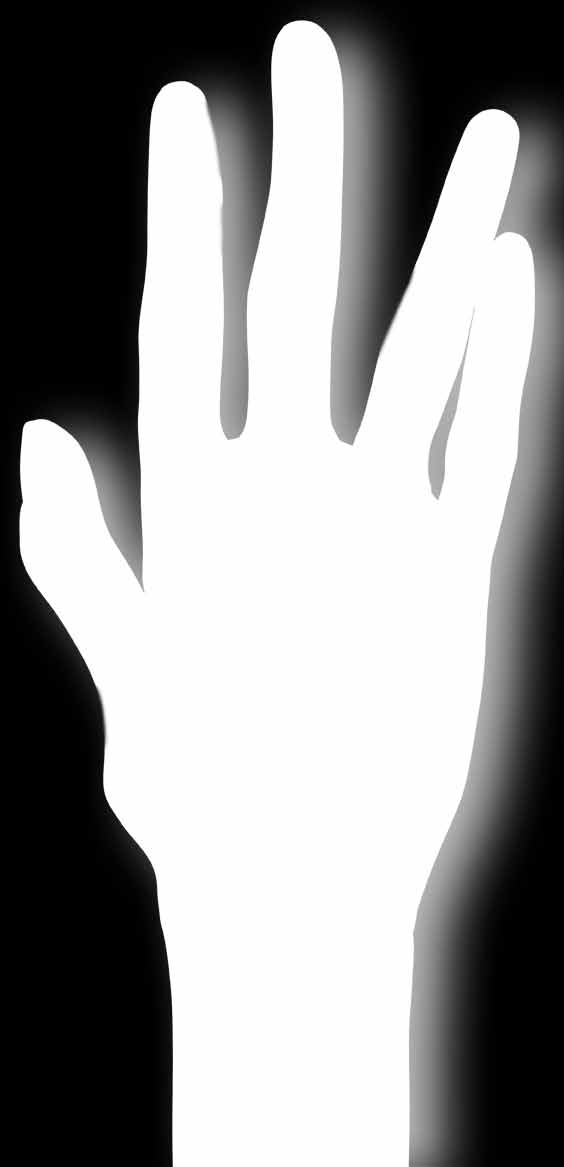
RA exhibits a predominance of inflammation in the small
progressing disease appeared. Thus, they could not be
joints affecting the hands and the feet, particularly
used to identify patients who would likely benefit from
the metacarpal phalangeal (MCP) joints, the proximal
early intervention. Nevertheless, these criteria are useful
interphalangeal joints (PIP), and the metatarsal
in identifying RA at the stage when patients often first
phalangeal (MTP) joints. Over 90% of patients have
see their clinician.13
involvement in those joints at some point in their
disease. That is followed by inflammation in the ankle,
• Morning stiffness with pain in and around the joints
the wrist, the subtalar region, the knees, and the
lasting at least one hour before maximal improvement
shoulder. Less commonly involved joints include elbows,
(removed from the new criteria but still useful)
hips, the acromioclavicular joint, the cervical spine, the
• Arthritis of the hand joints with at least one swollen
temporomandibular joint, and the cricoarytenoid area.
area in a wrist or the metacarpal phalangeal or
In contrast, OA has a predilection for the knees, the
proximal interphalangeal joint of a hand
hips, the lumbar spine, and the cervical spine.There is an
• At least 3 joint areas simultaneously affected by soft
overlapping spectrum of RA and OA joint distribution
that includes the knees, the first metatarsal phalangeal
• The presence of symmetrical arthritis, which is the
joint of the feet, and the cervical spine, although
simultaneous involvement of similar joint inflammation
rheumatoid arthritis involvement in the cervical spine
on both sides of the body (such as bilateral
is preferential for the first cervical vertebrae at the
involvement of the proximal interphalangeal joints
atlanto-axial articulation. Common locations of OA in
or the other joints shown in Figure 2); commonly,
the hands are in the distal interphalangeal joints, the
absolute symmetry is not present
PIPs, and particularly at the base of the thumb in the
first carpometacarpal joint, the predominant area of OA
• The presence of rheumatoid nodules over bony
throughout the skeleton.
prominences, extensor surfaces, or around joints
• Demonstration of abnormal amounts of serum RF
Clinical features of RA include characteristic radiographic
by any of the common methods in which the result
abnormalities on the anterior posterior hand and wrist
has been positive in less than 5% of normal
radiographs. Rheumatoid arthritis can progress to include
control subjects
bony erosions and bone decalcification localized or
adjacent to the involved joints. Many patients may have
• X-ray findings showing the presence of bone erosion
not progressed to the point of developing RA-associated
or bone decalcification adjacent to joints involved
radiographic changes when they seek medical assistance;
(removed from the new criteria due to the emphasis
if that is the case, with aggressive therapy, the physician
on early diagnosis)
can help the patient partially or completely circumvent
these types of manifestations.
Rheumatoid nodules are another characteristic of
this condition.9 Subcutaneous nodules appear over
Rheumatoid Arthritis Joint Distribution
bony prominences on the extensor surfaces such as
the proximal forearm. Typically soft and nonpainful,
Temporomandibular (30%)
Cervic l
a spine ( 40%)
rheumatoid nodules can be confused with gouty
tophi, which are typically firmer and are composed of
monosodium urate crystals. Rheumatoid nodules occur
later in the course of RA and are found in approximately
Hip (50%)
20% of patients with RA in the presence of seropositivity
Wrist (80%)
MCPs, PIPs (90%)
for RF.14
Knee (80%)
MTPs (90%)
Adapted from Gordon, DA, Hastings DE. In Rheumatology. 3rd ed. New York, NY:Mosby;2003:765-780.
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
DiFFEREnTiaTing Ra FRom oa
Clinical features of OA increase as the population ages.
Morning stiffness, in contrast to RA, is less than one hour,
Osteoarthritis is generally the most common diagnosis
and often under 30 minutes. There is inflammation early
when patients of any age present with chronic joint
in the course, although it is considerably less significant
pain, and RA is often misdiagnosed as OA in the early
than that seen with RA or with crystalline arthritis. Soft
stages. PCPs can differentiate rheumatoid arthritis
tissue swelling is also generally mild and variable. Bone
from osteoarthritis based on a variety of physical exam
enlargement results from bone spurs. This can lead
findings and laboratory parameters as measured over
to alignment changes and joint instability. Crepitus of
time. (See Figure 3.)
the joints is present on examination, and systemic and
constitutional features are usually absent.
How to Differentiate Rheumatoid
There is a progression of joint changes in OA. Early
irregular joint space narrowing occurs. Later, erosions
of the surfaces of the articular cartilage, subchondral
bone condensation, the development of bone spurs, and
Age of Onset
Starts in early adulthood;
peak incidence in 70s
Increases with age
cartilage fibrillation and clefts result from the destructive
Risk Factors
Trauma, orthopedic procedures
changes of osteoarthritis.
Morning stiffness of at least
1 hour and unexplained synovitis
Pain increases with use
and as day progresses
The changes of RA over time include gradual joint
DIPs, PIPs, base of
manifestations on radiograph. Progressive changes in
MCPs, PIPs, wrists, MTPs,
large joints; not usually DIPs
thumb (CMCs), knees, hips
late stage RA begin with soft tissue swelling, thinning
Soft tissue swel ing, warmth,
Osteop ytes
o y enlarge
So t t ssue s e
of the radial side of the cortex, minimal joint space
Osteopenia, erosions,
Osteophytes, subchondral sclerosis,
narrowing, and ultimately erosion of the bone just
uniform joint space narrowing
asymmetrical joint space narrowing
outside of the joint. The direction of forces in the hand
Lab Findings
Increase in ESR, rheumatoid factor,
and anti-CCP antibodies; anemia
along with active long-standing inflammation can lead to
subluxation of the metacarpal heads and ulnar deviation
of the hands, which is a characteristic manifestation
of later-stage RA.
RA has an earlier onset compared with OA. There are
certain immunogenetic and environmental risk factors
ETiology, PhysiCal Exam,
that may predispose to RA. Risk factors for OA include
being a woman, aging, strong family history, certain
anD lab WoRk
metabolic and endocrine factors, prior trauma and sports
RA is primarily a clinical diagnosis, as there is no single
injury including chronic biomechanical stress, and prior
test for the disease. Symptoms are highly variable in
inflammatory joint disease or joint infection.
number and severity from person to person; the full
In contrast to osteoarthritis, RA is frequently
range of symptoms develops over time with often only
characterized by morning stiffness, often exceeding one
a few present in the early stages; and other conditions
hour. In RA, there is evidence of soft tissue inflammation,
must often be ruled out in a process that eats into critical
swelling, warmth, and redness around the joints (see
time. However, in general, when the patient workup
previous section for information on joint involvement of
includes a positive family history of arthritis, evidence of
RA vs OA). While these may also present early in OA,
joint inflammation on exam, and elevated measures of an
the hallmark of osteoarthritis is the presence of bony
inflammatory and immunogenic process on blood testing,
osteophytes, which are often nontender and noninflamed
rheumatoid arthritis is the most likely diagnosis.
later in the course.
While the cause of RA is unknown, there are etiologic
Radiographically, RA shows osteopenia around the joint
associations. Rheumatoid arthritis is an autoimmune
with the ultimate development of periarticular bone
disease triggered by an unknown environmental factor in
erosions in joint space narrowing. In osteoarthritis, bone
a genetically predisposed individual. Infectious etiologies
spurs, or osteophytes, are seen as well as subchondral
have been implicated; however, no specific inciting agent
sclerosis, which is a thickening of the bone just beneath
has yet been identified. There is a strong genetic link
the joint space. Narrowing of the joint space also occurs.
between rheumatoid arthritis and the HLA system. There
In rheumatoid arthritis, there is elevation of acute
are also strong relationships with various environmental
phase, inflammatory mediators such as the erythrocyte
risk factors, in particular tobacco smoking, and a strong
sedimentation rate (ESR) and the C-reactive protein
female gender association, with RA being 3 times more
(CRP). RF and anti-CCP antibodies may be positive, and
prevalent in women.
there can be anemia of chronic inflammation. None of
Research demonstrates that ethnicity is usually an
these features are typically present in OA.
important factor in the level of disability and pain in
RA. One study showed that African American and
Hispanic patients with RA are more than twice as likely
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
as Caucasian patients to report some level of disability
onset occurs more rapidly over days to weeks. In 8-15%
in performing activities of daily living. These differences
of patients, symptoms begin within a few days of a
were related to the presence of comorbid conditions,
specific inciting event, such as an infectious illness.18
functional limitations, unhealthful behaviors, and lack
of health insurance. In another study, pain was worse
Table 2 outlines basic evaluation of disease for when a
in both African American and Hispanic groups (p<.01)
patient presents with symptoms consistent with RA. In
compared to Caucasians. A third study found that African
addition, a self-report questionnaire, such as the Health
American patients actually had fewer subcutaneous
Assessment Questionnaire (HAQ)19 and the Arthritis
rheumatoid nodules and tender joint counts than did
Impact Measurement Scales (AIMS)20 can be useful tools
Caucasian patients, but this did not seem to make any
in assessing disease progression and its impact on the
differences in disease outcome.15-17
patient's daily life.
Patients commonly present with pain and stiffness in
multiple joints, although one-third of patients initially
experience symptoms at just one location or a few
scattered sites. In most patients, symptoms emerge
over weeks to months, starting with one joint and often
accompanied by prodromal symptoms of anorexia,
weakness, or fatigue. In approximately 15% of patients,
Table 2. Evaluation of Disease9
Degree of joint pain
Duration of morning stiffness
Duration of fatigue
Limitation of function
Actively inflamed joints (tender and swollen joint counts)
Mechanical joint problems: loss of motion, crepitus, instability, malalignment,
and/or deformity
Erythrocyte sedimentation rate
C-reactive protein level
Complete blood cell count**
Hepatic enzyme levels (AST, ALT, and albumin)**
Synovial fluid analysis†
Functional status or quality of life assessments using standardized questionnaires
(physician's global assessment of disease activity, patient's global assessment of disease
activity, HAQ, AIMS, etc)
Radiographs of selected involved joints‡
*Performed only at baseline to establish the diagnosis. If initially negative, may be repeated 6-12 months after disease onset. **Performed at baseline,
before starting medications, to assess organ dysfunction due to comorbid diseases. †Performed at baseline, if necessary, to rule out other diseases. May
be repeated during disease flares to rule out septic arthritis. ‡Helps to establish a baseline.
AST: aspartate aminotransferase. ALT: alanine aminotransferase.
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
PRognosTiC FaCToRs
Biologic DMARDs include etanercept, infliximab,
adalimumab (which target tumor necrosis factor alpha),
Predictors of poor outcomes in the early stages of RA
and newer biologic DMARDs abatacept, rituximab, and
include a relatively low functional score on the HAQ early
tocilizumab. These are often used in conjunction with
in the disease progression, lower socioeconomic status,
nonbiologic DMARDs. The biologic DMARDs have a
lower educational level, strong family history of the
generally favorable benefit-risk profile overall despite
disease, and early involvement of many joints. Prognosis
some concern for an increased risk of infection and
is worse in patients who have a high ESR or CRP level
potentially a heightened risk of malignancy, with more
at disease onset, positive RF, presence of anti-CCP
studies under way to further delineate these risks in large
antibodies, and features of strong disease activity (eg,
high swollen joint count at onset, carriership of HLA-DR4
"Shared Epitope" alleles, or early radiologic changes).10
Current DMARD guidelines from the ACR recommend13
If not treated aggressively, RA has been associated with
• Single DMARD Therapy. Methotrexate or leflunomide
increased mortality. Historically, patients with RA can
as initial therapy for most patients with RA
die prematurely, on average 10 years earlier than age-
and sex-matched persons without rheumatoid arthritis.
• Dual DMARD Therapy. Methotrexate plus
Prognosis has improved with an earlier and more
hydroxychloroquine for patients with moderate to high
aggressive therapeutic approach.
disease activity
• Triple DMARD Therapy. Methotrexate plus
hydroxychloroquine plus sulfasalazine for patients with
TREaTmEnT
poor prognostic features and moderate to high levels
of disease activity
It is important to treat RA early. Three-quarters of
patients with early RA develop joint erosions within the
• Anti-TNF DMARDs. Anti-TNF drugs (etanercept,
first 2 years of symptom onset.21 Early treatment of
infliximab, adalimumab, golimumab, or certolizumab)
rheumatoid arthritis with DMARDs decreases the rate
for patients with established RA (more than 3 months'
of joint damage compared with delayed DMARD use
duration) who have not been helped by methotrexate;
and improves remission rates and patient outcomes.22
for patients with early RA (less than 3 months), reserve
Although NSAIDs improve signs and symptoms, they do
anti-TNFs (along with methotrexate) only for those
not slow or halt radiographic progression. DMARDs are
patients with high disease activity who have never
effective in this way and also result in less joint damage
received DMARDs
and deformity over time. Nonpharmacologic therapies
• Other Biologic DMARDs. Abatacept, rituximab, and
should complement the use of pharmacologic agents in
tocilizumab should be reserved for patients with at
RA. The use of the allied health professionals, including
least moderate disease activity and poor disease
physical therapists to maximize mobility and function,
prognosis who were not helped by methotrexate and
and occupational therapists to assist in improving
other nonbiologic DMARDs
hand function, can be very useful to people who have
functional impairments in their upper extremities.
Please see Table 3 on pages 9-10 for more information
on individual DMARDs.
EULAR guidelines recommend that, for early arthritis
in more than one joint, the physician should begin
treatment with DMARDs and refer the patient to
a rheumatologist within 6 weeks after the onset of
symptoms.23 "Tight control" of inflammation—using
disease activity scores and HAQs19, 20, 24 along with single
or multiple DMARDs—provides the patient with the best
chance for decreased joint damage and a more functional
life.25, 26
Nonbiologic DMARDs include methotrexate,
hydroxychloroquine, sulfasalazine, and leflunomide,
with methotrexate being the most commonly used. It
is available as either an oral weekly administration or in
parenteral forms with a dose range of between 7.5 mg
and 25 mg once weekly. Because methotrexate reduces
levels of folic acid (folate) in the body, it is necessary to
prescribe folic acid supplements to prevent side effects.27
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
Table 3. Monitoring DMARDs Used for RA13, 18, 28, 29
Common: Mild to moderate infusion reactions;
None unless
Effective in patients who are
increased risk for bacterial infection (especially in
patient also receiving
nonresponsive to methotrexate and in
patients with underlying lung disease)
other DMARDs
patients who have failed to respond to
Rare: Infections; possible increased risk for cancer
• Discontinue in case of active infection
Common: ISRs (20%) based on clinical trials;
None unless
Highly effective for
increased risk for bacterial infection
patient also receiving
moderate to severe disease
Rare: Opportunistic infection; reactivation of TB;
other DMARDs
• Adalimumab and other TNF inhibitors lupus-like reactions; possible increase in lymphoma
are not recommended in patients
not yet determined; CHF symptoms; demyelination
with demyelinating disease or with
congestive heart failure
• Discontinue in case of active infection
Common: Upper respiratory tract infection;
Test for latent TB
For moderate to severe RA in
nausea; abnormal liver tests; redness at injection
before prescribing;
combination with methotrexate
site; hypertension; bronchitis; dizziness; sinusitis;
monitor for TB
• Discontinue in case of active infection flu; fever; cold sores; numbness or tingling
Rare: Opportunistic bacterial and fungal infections
including TB and bacterial sepsis; lupus-like
symptoms; psoriasis; allergic reactions; lymphoma;
demyelinating disease; heart failure
Cyclosporine (Gengraf®, Neoral®,
Common: Bleeding, tender, or enlarged gums;
Creatinine every
or generic)
increase in hair growth; trembling and shaking of
2 weeks until dose is
• Use in patients who have not
stable, then monthly;
responded to other drugs
Rare: Hypertension; renal disease; sepsis
consider CBC,
• Do not take live vaccines while
LFTs, and potassium
on this drug
level tests
Common: ISRs (37%); increased risk for bacterial
None unless
Effective for moderate to severe disease and fungal infections; pain or burning in throat;
patient also receiving
• Etanercept and other TNF inhibitors
runny or stuffy nose
other DMARDs
are not recommended in patients
Rare: Opportunistic infection; reactivation of TB;
with demyelinating disease or with
lupus-like reactions; possible increase in lymphoma
congestive heart failure
not yet determined; demyelination
• Discontinue in case of active infection
Common: Upper respiratory tract infections;
Evaluate for
For moderate to severe RA in
nasopharyngitis; headache; hypertension;
TB before
combination with methotrexate
• No live vaccines
Rare: Opportunistic infections; lipid elevations;
• Discontinue in case of active infection hepatic transaminase elevations; gastrointestinal
(GI) perforation secondary to diverticulitis;
neutropenia; thrombocytopenia; CHF; lymphoma;
Common: Diarrhea; bloating; anorexia; rash;
Effective for mild disease and in
headache; nausea or vomiting; stomach cramps
combination with methotrexate
Rare: Retinopathy, macular damage (if dosed too
high); neuromyopathy
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
Table 3. Monitoring DMARDs Used for RA13, 18, 28, 29
Common: ISRs (20%); increased risk for bacterial None unless
Effective for moderate to severe disease
infection; abdominal pain; cough; dizziness;
patient also receiving
• Infliximab and other TNF inhibitors
fainting; headache; muscle pain; runny nose;
other DMARDs
are not recommended in patients
shortness of breath; sore throat; vomiting;
with demyelinating disease or with
Evaluate for TB before
congestive heart failure
Rare: Opportunistic infection; reactivation of TB;
• Discontinue in case of active infection
lupus-like reactions; possible increase in
lymphoma not yet determined; demyelination
Common: Diarrhea; nausea; alopecia; anorexia;
CBC, LFT, and serum
For moderate to severe disease
rash; elevated LFT levels; teratogenic;
creatinine levels every
• Contraindicated in potentially
leukopenia; bloody or cloudy urine; congestion
2-4 weeks under
in chest; cough; difficult, burning, or painful
3 months, every
• Discontinue in case of active infection
urination; fever; headache; heartburn; loss of
8-12 weeks at 3 to
appetite; stomach pain; sneezing; sore throat
6 months, and every
Rare: Severe hepatotoxicity; pulmonary fibrosis
12 weeks after
Common: Nausea; diarrhea; alopecia; fatigue;
CBC, LFT, and serum
Well-tolerated; gold standard
lassitude; headache; elevated LFT levels;
creatinine levels every
for managing RA
mouth ulcers; rash
2-4 weeks under
• Contraindicated in potentially
Rare: Hepatotoxicity; pneumonitis; cytopenias;
3 months, every
sepsis; Epstein-Barr; nodulosis
8-12 weeks at 3 to
• Discontinue in case of active infection
6 months, and every
12 weeks after
Common: Mild to moderate infusion reactions;
CBC and platelet
Effective in long-standing, active RA
increased risk for bacterial infection; abdominal counts should be
with inadequate response to TNF
pain; chills/shivering; fever; headache; itching
obtained at regular
antagonist therapy when used in
Rare: Severe infusion reactions; medications and intervals, and
combination with methotrexate
supportive care measures should be available
more frequently
• Discontinue in case of active infection during infusion; repeat administration may be
in patients who
associated with lower immunoglobulin levels
Common: Abdominal pain; aching joints;
CBC, LFT, and serum
Effective for mild to moderate disease
diarrhea; headache; sensitivity to sunlight; loss
creatinine levels every
• Contraindicated in patients who have
of appetite; nausea or vomiting; skin rash
2-4 weeks under
Rare: Cytopenias; hepatotoxicity
3 months, every
8-12 weeks at 3 to
6 months, and every
12 weeks after
Common: Upper respiratory tract infections;
Test for latent TB
Effective in combination with
nasopharyngitis; headache; hypertension;
before prescribing;
methotrexate or other nonbiologic
monitor for TB;
DMARDs for moderate to severe RA
Rare: Opportunistic infections; lipid elevations;
in patients who have not responded to
hepatic transaminase elevations; GI perforation
1 or more anti-TNF therapies
secondary to diverticulitis; neutropenia;
• Live vaccinations should not be
• Contraindicated in potentially
childbearing women
• Do not administer to patients
with active infection
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
The injectable anti-TNF agents are commonly taken once
The goal of RA treatment, at any time during its course,
weekly or once every 2 weeks; intravenous anti-TNF
is to achieve a low disease activity state or clinical
agents are commonly given every 2 months, or monthly
remission. Complete clinical remission is defined by
for abatacept and tocilizumab, and even less frequently
the ACR as the presence of at least 4 of the following
for rituximab at only once or twice a year. Biologic
criteria for at least 2 consecutive months:
DMARDs should not be taken by patients with active
bacterial infections, active herpes-zoster viral infection,
• Morning stiffness less than or equal to 15 minutes
active or latent tuberculosis, or active hepatitis B or C.
Screening for both hepatitis B and C is reasonable for
• No fatigue
all patients under consideration for any DMARD. Those
• No joint pain
with chronic viral hepatitis may still have their comorbid
• No joint tenderness or pain on motion
rheumatic disease aggressively treated, depending on
their condition, and there is evidence to suggest that,
• No soft tissue swelling in joints or tendon sheaths
in the setting of chronic hepatitis C, anti-TNF therapy
• ESR less than or equal to 30 in females and
is not only safe, but may also substantially improve
20 in males
the tolerability of antiviral therapy with interferon and
ribavirin, thereby boosting the hepatitis cure rate.30
Because traditional DMARDs take several months to
True remission means that the patient has no signs of
provide efficacy, low dose oral glucocorticoids (steroids)
active inflammation after all medications are stopped,
are often used as a bridge therapy during this time
which is still an uncommon outcome in RA. Therefore,
to control signs and symptoms of inflammation and
the goal is to decrease disease activity to the lowest
maintain adequate physical function. Unfortunately,
level, defined as few tender or swollen joints, little
many DMARDs tend to lose effectiveness over time.
fatigue, full function, and a normal ESR and CRP
Combining DMARDs with each other or with drugs in
level while the patient is receiving medications (eg,
other categories offers the best approach for many
methotrexate).25, 32 When disease remains uncontrolled,
patients. The addition of a glucocorticoid to any
further evaluation of involved joints beyond plain
combination may also be helpful.
radiographs might include MRI and ultrasonography,
which can pick up RA bone erosions. These tests can
Monitoring for efficacy and adverse events is required
provide early warning signs of a more aggressive illness
for all these drugs, especially the nonbiologic DMARDs.
and a need for increased therapeutic aggressiveness.19-21
CBC, creatinine, and liver function tests, particularly
in the case of methotrexate, should be performed
Lastly, the ACR has endorsed 7 quality indicators that
regularly (see Table 3 on pages 9-10) while patients are
pertain to management of patients with RA.33, 34
on these therapies to detect early abnormalities and to
make adjustments in medication dose as needed. Some
DMARDs may produce gastrointestinal side effects,
and, over the long term, each poses some risk for rare
but serious complications, such as bacterial and fungal
infections, lymphoma, or heart failure. (In some cases,
however, they may be less harmful than long-term
NSAID treatment.)
Nonpharmacologic interventions are also important
in the management of RA. There is excellent quality
evidence to suggest that exercise provides significant
functional benefits in patients with RA, together
with important cardiovascular benefits such as
improvements in lipid profile and insulin sensitivity,
reduction of prothrombotic states and body fat
content, and diminished risk of death from
cardiovascular disease (CVD).31
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
sCREEning FoR ComoRbiDiTiEs
EDuCaTing PaTiEnTs anD CaREgivERs:
anD aDvERsE TREaTmEnT EFFECTs
EviDEnCE-basED PaTiEnT ChoiCE
Fatigue, low-grade fever, and weight loss are
There is an international increase in awareness
manifestations of systemic inflammatory disease. These
that patients are not only able, but should also be
symptoms are not specific for RA and can occur in other
encouraged, to play an important role in deciding
conditions that involve inflammation, infection, or even
on their care, in defining ideal care, and in generally
malignancy. If not treated aggressively, RA has been
improving healthcare delivery. This trend is reflected
associated with increased mortality. Historically, patients
in a host of new concepts like patient-centered
with rheumatoid arthritis can die prematurely, on average
care, patient empowerment, patients as partners,
10 years earlier than age- and sex-matched persons
shared decision making, and informed choice. Patient
without rheumatoid arthritis. Prognosis has improved with
autonomy is increasingly being regarded as a basic
an earlier and more aggressive therapeutic approach.
value and an important goal in health care, as well as
the key to better adherence to advice and treatment
Rheumatoid arthritis has significant associated
and, therefore, to better health outcomes.
comorbidities, which complicate diagnosis and treatment.
CVD is the most prevalent comorbidity and most common
The notion of "evidence-based patient choice" simply
cause of death in patients with RA (associated with
refers to the requirement that patients' treatment
17-42% of patient deaths)8 for reasons as yet unclear.31
choices be based on adequate evidence that a certain
Many of the medications used for RA, however, can
line of treatment will be the most effective in the
significantly impact common CVD risk factors, including
patient's particular situation. The issue, therefore, is not
the potential cardiovascular effects of commonly used
simply that of a sound choice in general, but a choice
NSAIDs, the hypertensive effects of some DMARDs
that is individualized for this particular patient in his or
(eg, cyclosporine and leflunomide), and potential
her particular circumstances. Studies have shown that
beneficial lipid effects of others (eg, hydroxychloroquine).
patients with RA who are well informed and participate
Other major comorbidities associated with death in
actively in their own care have less pain and make fewer
patients with RA include infections (9-24%), renal disease
visits to the doctor than do other patients with RA.
(8-10%), pulmonary disease (7-10%), and gastrointestinal
Becoming an informed consumer of medical information
disease (4-10%).6 Raised levels of systemic inflammation
often empowers a patient to take control of his or
have also been shown to predispose patients to
her illness.
developing diabetes. Other common comorbidities
Thanks to the Internet, patients are much better
include an increased risk of fracture, an increased
informed, possessing important information they need
risk of cancer (particularly lymphoma), and higher
to share with their healthcare professionals. Patients'
rate of infections. Patients with rheumatoid arthritis
information needs differ considerably from those of
should undergo aggressive cardiovascular risk factor
their physicians and other healthcare professionals, a
management, evaluation of their bone density, and
fact that is often misunderstood, yet the effectiveness
periodic and appropriate cancer screening.
of treatment depends on the cooperation of the patient
In addition, because patients with RA have a 6- to
who is a willing member of the caregiving team.35 The
PCP's and rheumatologist's job is to provide additional
9-fold increase in the rate of serious infections,6
supportive help and information.
tuberculosis testing and influenza and pneumococcal
vaccinations are recommended, although titers may
Nevertheless, studies show that many patients do not
be lower. Live vaccines (including the zoster vaccine
understand what their doctors have told them and do
for shingles) should be avoided in patients on steroids
not participate in decisions about their care, leaving
and other immunosuppressive therapies, including
them ill-equipped to make daily decisions and take
methotrexate, leflunomide, and biologics due to
actions that lead to good management. Other patients
are unaware that taking an active role in managing their
condition can have a big impact on how they feel and
The PCP needs to be extra vigilant when providing
what they are able to do. Enabling patients to make
ordinary medical care for patients with RA as typically
good choices and sustain healthy behaviors requires a
recognized signs and symptoms of influenza, infection,
collaborative relationship between healthcare providers,
or other commonly seen conditions may be masked by
their teams, patients, and their families so that patients
RA treatment. Symptomatic fevers indicating
can build the skills and confidence they need to lead
inflammation may be lower than normally seen, and a
active and fulfilling lives.36
critical diagnosis may thus be missed. Certain conditions
also require the withholding of DMARD or other
treatment while the coexisting illness runs its course.
Communication between the PCP and rheumatologist
is essential to ensure that the patient is appropriately
treated for RA and for other ailments either comorbid,
a complication, or randomly contracted.
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
Patient education and arthritis self-management
using ThE ChRoniC DisEasE moDEl
programs, as well as support groups, help people to
oF CollaboRaTivE CaRE
become better informed and to participate in their
own care. An example of a self-management program
Rheumatoid arthritis is a chronic disease. It cannot be
is the Arthritis Self-Help Course offered by the Arthritis
cured; it can only be managed. Flare-ups happen, and
Foundation. Self-management programs teach about
the course of the disease is often characterized by
rheumatoid arthritis and its treatments, exercise and
good days and bad. Patients require multidisciplinary
relaxation approaches, communication between patients
support throughout their lives from PCPs, nurses and
and healthcare providers, and problem solving.37 Research
nurse practitioners, specialists, allied health professionals
on these programs has shown that they help people
including occupational and physical therapists, community
advocates, and patient support groups.
• Understand the disease
A number of practice models have arisen to deal with
the complexities, multidisciplinary care, and routine
• Reduce their pain while remaining active
monitoring required for optimal management throughout
• Cope physically, emotionally, and mentally
the course of a chronic disease.38 Among them are the
• Feel greater control over the disease and build a
chronic care model,39 the patient-centered medical
sense of confidence in the ability to function and
home,40 care coordination, shared management support,36
lead full, active, and independent lives
collaborative team-based care, case management, and
variations. Use of these models has spread slowly, with
the most experience coming in diabetes, asthma, and
Research has indicated that patients with RA find a one-
cardiovascular care. The variety and range of potential
to-one format helpful for learning about very specific
complications and adverse events associated with RA
information such as medications, whereas a group
make it a prime candidate for collaborative management
format was better for learning about self-management
and patient-centered care models, when available.
techniques and exercise.31 Leaflets were viewed as
helpful and a useful memory aid, but insufficient alone to
As can be expected, no one model fits all, and
address the breadth of patients' concerns. A comparison
practitioners have a rich field for mixing and matching
of group education with supporting self-help guide vs
elements of these models to fit their situations. Rural
supporting self-help guide alone showed improvement
physicians with rare access to specialists are beginning
in self-efficacy in the former group, whereas no
to use telemedicine models for consultation and other
changes were observed in the latter group. Conversely,
assistance in caring for their patients with rheumatoid
questionnaire research has shown the preferred format
arthritis.41 Medicare, Medicaid, and other government
for learning about arthritis was in writing.
health programs have been reimbursing doctors and
hospitals that provide care remotely to rural and
Concordance, the informed interaction in the
underserved areas. Although the ACR does not support
individualized decision-making process in the patient–
use of the patient-centered medical home at this time42
professional partnership, promotes shared responsibility
(due to questions about the relative roles of specialists,
for care and is particularly important for successful
primary care physicians, and allied health personnel
lifestyle modification interventions and for preventive
within the model), evidence-based care points to the
therapy.31 A 2002 survey of more than 2000 patients
need for management of arthritis as a chronic disease
with diabetes revealed that two-thirds of respondents
with interventions directed to the reduction of pain and
did not consider CVD a serious complication of diabetes,
prevention of disability as well as timely and appropriate
suggesting that their education on, and communication
access to specialist care.38
of, CVD risk had been inadequate. Such shortcomings
are likely to be more pronounced in patients with
Collaboration and communication among the range of
RA, where research evidence about the nature of the
healthcare professionals, patients, and family members
various risks has only recently started to reach the
are essential for optimal patient health, therapeutic
medical, let alone the patient, communities. Indeed,
concordance, and quality of life. The use of teams to
previous work has shown that only a quarter of patients
manage arthritis care is a long-standing tradition in some
with RA and confirmed CVD recorded the latter as a
countries and has been shown to be effective in improving
comorbidity when listing their other illnesses. Therefore,
patient outcomes.38 However, despite the increased
a combination of research findings, management
interest in exploring models of care for arthritis, there is a
imperatives, observations, and experience from other
dearth of literature examining models in different settings.
conditions and from RA, as well as common sense, place
patient education on the cardiovascular aspects of
The ACR, in effect, endorses a chronic care model for
rheumatoid disease right at the center of any successful
management of RA when its guidelines recommend that
a general health maintenance strategy be developed,
with responsibility coordinated among the patient's
healthcare providers. "Routine prevention measures,
such as screening for hypertension or cancer, should be
recommended and risk factors modified."9
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
The PCP is critical to implementing the chronic care
model, monitoring the effects of treatment, managing
comorbidities and ordinary illness, ensuring patient-
Case 1: LP is a 60-year-old dental hygienist with a
centered care, and effectively collaborating with the
2-month history of pain in the base of her right thumb.
team of physicians, nurses, physical and occupational
She has had intermittent enlargement of scattered
therapists, and other healthcare professionals necessary
bilateral distal interphalangeal joints over the past 5 to
to maintain and optimize the patient's quality of life
6 years. She has used ibuprofen occasionally without
relief, causing mild stomach irritation. Her past medical
and activities of daily living, with the ultimate goal of
history is unremarkable. Her family history is notable in
complete clinical remission. Resources regarding the
that her 90-year-old mother had developed bumps on
implementation of new practice models, collaborative
her hands in her 60s. Her physical examination revealed
chronic care, and the medical home are proliferating,
and their use is encouraged to benefit healthcare
professionals and the patient in navigating the
Question 1: Based on the information presented so far,
complicated waters of RA treatment.40, 43
which of the following diagnoses should be considered?
Whether isolated in a rural area or part of a busy
A. Psoriasis
urban practice, the PCP is ultimately responsible for
B. Osteoarthritis (primary or secondary)
ensuring that the patient with RA is appropriately
diagnosed, treated, and monitored throughout the
course of their illness and other illnesses they may
D. Rheumatoid arthritis
face whose treatment is affected by the underlying
rheumatoid disease. Even if the patient decides to see
the rheumatologist for complaints other than RA, the
F. Carpal tunnel syndrome
PCP should work with the specialist to ensure optimal
Answer: A, B, and C. Psoriasis, osteoarthritis, and
patient care as long as the patient is still registered with
chondrocalcinosis are the most likely diagnoses at this
the PCP's practice. Regular contact with the patient
point. The presence of nontender bony enlargement on
to answer questions, provide preventive services, and
the distal interphalangeal and proximal interphalangeal
monitor the effects of treatment can make a huge
joints in the absence of synovitis makes rheumatoid
difference in individual patient outcomes.
arthritis unlikely. The absence of findings consistent
with psoriasis on physical exam make the diagnosis
of psoriatic arthritis unlikely. There are currently no
commercially available diagnostic laboratory tests
for osteoarthritis.
Based on the physical examination of the patient,
radiographs of the hands are obtained. The radiographs
indicate irregular joint space narrowing, the presence
of marginal osteophytes or bone spurs, as well as
subchondral sclerosis, thickening of the bone just beneath
the joint line, and cysts in the subchondral region.
Question 2: Based on the information presented so far,
which of the following diagnoses should be considered?
A. De Quervain's tenosynovitis
B. Psoriasis
C. Osteoarthritis (primary or secondary)
D. Chondrocalcinosis
E. Rheumatoid arthritis
F. Gout
G. Carpal tunnel syndrome
Answer: C. Osteoarthritis is the most likely diagnosis,
based on the presence of irregular joint space narrowing,
osteophyte formation, and subchondral cysts. The x-rays
do not show any other major abnormalities that might
raise other diagnostic considerations.
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
Case 2: KC is a 38-year-old woman who complains of
Question 2: Based on the information presented so far,
wrist pain. She describes her pain as dull, constant,
you would order all of the following tests that would prove
and worse in the morning, but persistent throughout
helpful in the diagnosis/differential diagnosis EXCEPT
the day. She's also experiencing pain in her elbows and
feet, though less pain than in her wrist. She has had no
A. Erythrocyte sedimentation rate (ESR)
neurologic symptoms and no systemic complaints other
B. Creatinine kinase
than fatigue and difficulty sleeping. Her only relevant
C. Rheumatoid factor (RF)
past medical history is that of Graves' disease. She has
been using acetaminophen several times per day since
D. Radiography of her hand
her pain started one month ago, but it's providing only
E. Anti-CCP antibody
limited relief. She is also on levothyroxine. She believes
she might have carpal tunnel syndrome.
Answer: B. Creatinine kinase would not be useful in this
case. Information specific to a diagnosis of rheumatoid
Her family history is notable for fibromyalgia in her
arthritis and not osteoarthritis or other rheumatic
mother, but no family history of arthritis or systemic
diseases would come from the ESR, RF, anti-CCP, and
rheumatic disease. She smokes a half pack of cigarettes
hand x-ray.
per day. At her visit, she provides an x-ray of her
hand and wrist, which shows no abnormalities, and an
With a working diagnosis of undifferentiated
MRI scan of her wrist, which shows a lobulated mass
inflammatory arthritis, you start KC on a generic
representing a benign ganglion cyst.
nonsteroidal anti-inflammatory drug and provide her
with a 2-week course of methylprednisolone. She
Question 1: Based on the information presented so far,
returns in one month with complaints of pain in the
which of the following diagnoses should be considered
same joints, which have now worsened. Her wrists are
most strongly?
stiff for at least an hour in the morning, and they are
now clearly swollen, particularly in the finger joints,
A. Osteoarthritis (primary or secondary)
which are also painful. The second and third PIP joints of
both hands feels "mushy" to the touch, and soft-tissue
C. Early rheumatoid arthritis
swelling is present in the PIP and MCP joints in the
index and middle fingers. You obtain x-rays, which show
moderate osteopenia in cancellous bones, primarily
Answer: C. Early rheumatoid arthritis remains a strong
periarticularly, and thinning of the radial cortices of the
consideration. Gout is exceedingly uncommon in
metacarpal heads, but no bone erosions are seen. These
36-year-old premenopausal women. Osteoarthritis
are early changes of rheumatoid arthritis. An anti-CCP
is also unlikely based on her age, and the wrists are
autoantibody and rheumatoid factor returns positive
not a particular target for primary osteoarthritis.
with an ESR elevated at 78 mm/hr.
Fibromyalgia is a consideration given her family
Based upon these new symptoms, signs, and x-ray
history and sleep disturbance, but its typical hallmark
findings, the patient satisfies the older as well as the
is pain all over above and below the waist and both
newer classification criteria for rheumatoid arthritis.
sides of the body. Her pain is predominantly localized
While these criteria are most useful in conducting
to the wrists. Tendonitis can be a manifestation of
clinical trials and in ensuring a uniform case definition,
rheumatoid arthritis. In most cases of rheumatoid
they provide a framework to consider the major
arthritis, 3 or more joints will have soft tissue swelling or
manifestations of rheumatoid arthritis.
inflammation as observed by a physician. However, the
2010 classification criteria require arthritis in only one
Question 3: Your initial RA management plan is to start:
joint along with other features for the clinician to think
seriously about a referral to a rheumatologist to confirm
a diagnosis of RA. She does not have observable
B. Rituximab
rheumatoid nodules at this time.
C. Abatacept
D. Methotrexate
Answer: D. You would start her on methotrexate, which
is the most commonly used DMARD in the United States
and abroad. It is the first line of defense recommended
by ACR guidelines for treatment of RA because it is
most likely to induce a long-term response. The drug is
generally well tolerated and is frequently paired with
nonbiologics for enhanced efficacy. It is available as
either an oral weekly administration or in parenteral
forms with a dose range of between 7.5 and 25 mg
once weekly, making it easy to administer and facilitate
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
Case 3: WS is a 36-year-old female who presented
Ra REsouRCEs
with pain in both wrists, which seemed to become
noticeable after giving birth. She has been taking
acetaminophen with little relief. She has no other
The following Web sites are a few potential resources
systemic complaints except that she has noticed some
for further information. This list does not constitute
fatigue. In her history, she once had an MRI of her
endorsement or recommendation of any Web site by the
wrist due to pain and was diagnosed with a ganglionic
faculty, sponsor, or commercial supporters.
cyst. Exam reveals pain in her hands and wrists
on all passive and active range of motion. Tinel's,
Finkelstein's, and Phalen's maneuvers are all negative.
Neuromuscular strength and sensory exams are
American Academy of Orthopaedic Surgeons
all normal.
Her laboratory tests reveal an ESR of 42, CRP of 3.5,
American College of Rheumatology
and RF of 63 (all high). In addition, her ANA is also
slightly elevated at 1:160. X-rays of her hands and
wrists reveal soft tissue swelling of her MCP and
Improving Chronic Illness Care
PIP joints. There is no joint erosion noted on x-ray.
Management has been started with an NSAID being
added to her acetaminophen.
The TransforMED Patient-Centered Model
Question 1: Should she be referred to the rheumatologist
for diagnostic and therapeutic evaluation?
Answer: Yes. The patient can benefit from further
For Patients
examination and objective testing to make the early
and accurate diagnosis. If she turns out to have an
inflammatory arthritis, then aggressive treatment with
appropriate agents would lead to preservation of joint
structure and function. Regular consultation with the
The Johns Hopkins Arthritis Center
rheumatologist can ensure optimal patient care and
facilitate optimal patient outcomes.
National Institute of Arthritis and Musculoskeletal and
Question 2: The PCP and rheumatologist both treat RA
Skin Diseases (NIAMS)
using the chronic care model. Which of the following are
elements of the chronic care model?
Orthopaedic Web links
A. Collaborative care
B. Patient-centered approach
C. Evidence-based patient choice decision making
D. Treatment approaches designed to be
concordant with the patient's lifestyle
E. All of the above
Answer: E. The chronic care model employs all of these
elements to achieve better outcomes and patient
adherence, along with greater patient satisfaction
with the care process. When work flow is redesigned
around the needs and desires of the patient, the process
becomes efficient and driven by improved processes and
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
1. United States Bone and Joint Decade. The Burden of Musculoskeletal Diseases in the United States. Rosemont, IL:
American Academy of Orthopaedic Surgeons; 2008. Available at: http://www.boneandjointburden.org/.
Accessed September 10, 2010.
2. Helmick CG, Felson DT, Lawrence RC, et al. Estimates of the prevalence of arthritis and other rheumatic conditions
in the United States. Part I. Arthritis Rheum. 2008;58(1):15-25.
3. Dunlop DD, Manheim LM, Yelin EH, Song J, Chang RW. The costs of arthritis. Arthritis Rheum. 2003;49(1):101-113.
4. Arthritis Foundation. News from the Arthritis Foundation. Arthritis Prevalence: A Nation in Pain. Available at:
5. Yelin E, Callahan LF. The economic cost and social and psychological impact of musculoskeletal conditions.
National Arthritis Data Work Groups. Arthritis Rheum. 1995;38(10):1351-1362.
6. Weinblatt ME, Kuritzky L. RAPID: rheumatoid arthritis. J Fam Pract. 2007;56(4 Suppl):S1-S7.
7. NCHS. National Ambulatory Medical Care Survey. 1995.
8. Everts B, Wahrborg P, Hedner T. COX-2-Specific inhibitors--the emergence of a new class of analgesic and
anti-inflammatory drugs. Clin Rheumatol. 2000;19(5):331-343.
9. Centers for Disease Control and Prevention. Guidelines for the management of rheumatoid arthritis: 2002 Update.
10. Kountz DS, Von Feldt JM. Management of rheumatoid arthritis: A primary care perspective. J Fam Pract.
2007;56(10 Suppl A):59A-73A.
11. Suter LG, Fraenkel L, Holmboe ES. What factors account for referral delays for patients with suspected rheumatoid
arthritis? Arthritis Rheum. 2006;55(2):300-305.
12. Aletaha D, Neogi T, Silman AJ, et al. 2010 Rheumatoid arthritis classification criteria: an American College of
Rheumatology/European League Against Rheumatism collaborative initiative. Ann Rheum Dis. 2010;69(9):1580-
13. Saag KG, Teng GG, Patkar NM, et al. American College of Rheumatology 2008 recommendations for the use
of nonbiologic and biologic disease-modifying antirheumatic drugs in rheumatoid arthritis. Arthritis Rheum.
14. Wilke W. Rheumatoid Arthritis. Disease Management Project [http://www.clevelandclinicmeded.com/medicalpubs/
diseasemanagement/rheumatology/rheumatoid-arthritis/. Accessed September 27, 2010.
15. Bruce B, Fries JF, Murtagh KN. Health status disparities in ethnic minority patients with rheumatoid arthritis:
a cross-sectional study. J Rheumatol. 2007;34(7):1475-1479.
16. Mikuls TR, Kazi S, Cipher D, et al. The association of race and ethnicity with disease expression in male US veterans
with rheumatoid arthritis. J Rheumatol. 2007;34(7):1480-1484.
17. Song J, Chang HJ, Tirodkar M, Chang RW, Manheim LM, Dunlop DD. Racial/ethnic differences in activities of daily
living disability in older adults with arthritis: a longitudinal study. Arthritis Rheum. 2007;57(6):1058-1066.
18. Rindfleisch JA, Muller D. Diagnosis and management of rheumatoid arthritis. Am Fam Physician. 2005;72(6):1037-
19. Fries J, Stanford University School of Medicine. Health Assessment Questionnaire. http://www.chcr.brown.edu/
pcoc/EHAQDESCRSCORINGHAQ372.PDF. Accessed October 19, 2010.
AIMS2. Accessed October 19, 2010.
21. Emery P, Breedveld FC, Dougados M, Kalden JR, Schiff MH, Smolen JS. Early referral recommendation for newly
diagnosed rheumatoid arthritis: evidence based development of a clinical guide. Ann Rheum Dis. 2002;61(4):290-297.
22. Roberts LJ, Cleland LG, Thomas R, Proudman SM. Early combination disease modifying antirheumatic drug
treatment for rheumatoid arthritis. Med J Aust. 2006;184(3):122-125.
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Improving Early Diagnosis and Treatment
of Rheumatoid arthritis in Primary Care
23. Combe B, Landewe R, Lukas C, et al. EULAR recommendations for the management of early arthritis: report of
a task force of the European Standing Committee for International Clinical Studies Including Therapeutics
(ESCISIT). Ann Rheum Dis. 2007;66(1):34-45.
24. Disease Activity Score. http://www.das-score.nl/www.das-score.nl/. Accessed October 19, 2010.
25. Paget SA. Shared decision making in early arthritis: The physician's role. The Journal of Muskuloskeletal Medicine.
26. Mease PJ. Improving the routine management of rheumatoid arthritis: the value of tight control. J Rheumatol.
27. A.D.A.M. Inc. New York Times Health Guide: Rheumatoid Arthritis. Available at: http://health.nytimes.com/health/
guides/disease/rheumatoid-arthritis/diagnosis.html. Accessed September 21, 2010.
28. Bingham CO, 3rd, Miner MM. Treatment, management, and monitoring of established rheumatoid arthritis.
J Fam Pract. 2007;56(10 Suppl Rapid):S1-S7.
29. National Institute of Arthritis and Musculoskeletal and Skin Diseases. Handout on Health: Rheumatoid Arthritis.
Available at: http://www.niams.nih.gov/health_info/rheumatic_disease/. Accessed September 21, 2010.
30. Ferri C, Ferraccioli G, Ferrari D, et al. Safety of anti-tumor necrosis factor-alpha therapy in patients with
rheumatoid arthritis and chronic hepatitis C virus infection. J Rheumatol. 2008;35(10):1944-1949.
31. John H, Hale ED, Treharne GJ, Kitas GD. Patient education on cardiovascular aspects of rheumatoid disease:
an unmet need. Rheumatology (Oxford). 2007;46(10):1513-1516.
32. Ranganath VK. Through the looking glass: "remission" in rheumatoid arthritis. J Rheumatol. 2009;37(7):1371-1373.
33. Rheumatoid Arthritis Quality Indicators. http://www.rheumatology.org/practice/clinical/quality/RA.asp.
Accessed August 2, 2010.
34. Physician Consortium for Performance Improvement, American College of Rheumatology. Rheumatoid Arthritis
Physician Performance Measurement Set. Available at: http://www.ama-assn.org/ama1/pub/upload/mm/370/
rheumatoid-arthritis.pdf. Accessed September 21, 2010.
35. Moore W. Patient Autonomy and Evidence-Based Patient Choice: Philosophical and Ethical Perspectives
[Dissertation]. Stellenbosch, South Africa: Philosophy, Stellenbosch University; 2010.
36. Schaefer J, Miller D, Goldstein M, Simmins L. Partnering in Self-Management Support: A Toolkit for Clinicians.
toolkit_for_clinicians.pdf. Accessed September 10, 2010.
37. National Institute of Arthritis and Musculoskeletal and Skin Diseases. Handout on Health: Rheumatoid Arthritis.
Handout on Health [April 2009; http://www.niams.nih.gov/health_info/rheumatic_disease/:http://www.niams.nih.
gov/health_info/rheumatic_disease/. Accessed August 25, 2010.
38. MacKay C, Veinot P, Badley EM. Characteristics of evolving models of care for arthritis: a key informant study.
BMC Health Serv Res. 2008;8:147.
39. Kahn KL, MacLean CH, Liu H, et al. The complexity of care for patients with rheumatoid arthritis: metrics for better
understanding chronic disease care. Med Care. 2007;45(1):55-65.
40. Rosenthal TC. The medical home: growing evidence to support a new approach to primary care. J Am Board Fam
41. Vliet Vlieland TP, Li LC, MacKay C, Bombardier C, Badley EM. Current topics on models of care in the management
of inflammatory arthritis. J Rheumatol. 2006;33(9):1900-1903.
42. American College of Rheumatology Committee on Rheumatologic Care. American College of Rheumatology
Position Statement: The patient-centered medical home concept. Available at: http://www.rheumatology.org/
43. Rothman AA, Wagner EH. Chronic illness management: what is the role of primary care? Ann Intern Med.
2010 Physicians' Institute for Excellence in Medicine and CME Enterprise, Inc.
Source: http://www.physiciansinstitute.org/wp-content/uploads/2012/11/RA-Monograph.pdf
Q. What are metered-dose inhalers? A. These are devices that dispense medicines directly into the lungs, in the form of a mist oraerosol in a specific dosage. In an MDI, themedicine is suspended in a liquid and forced underpressure into a small canister fitted into a plasticcase. When the canister is pressed, a measureddose of the medicine is released through themouth-piece.
How do I know my drug treatment Is there a natural way of treating For osteoporosis information and support is working? osteoporosis and preventing fractures contact our Helpline: It is difficult to know if a treatment is rather than using drugs? 0845 450 0230 or 01761 472721