Hiv/aids in the context of other global challenges
An executive summary for tackling global challenges
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS, 8-10 June 2011
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
Global2015 e. V. is an independent, non-profit and non-partisan association, registered under German law.
Its mission is to provide a comprehensive analysis and survey of the most urgent global challenges for human needs and life, and to encourage further action in tackling challenges such as world nutri-tion, climate change, and epidemics.
Members of the board of directors: Sarah Hartnett LL.B. (Ling.Germ.), Dipl.-Pol. Lars VogelsangSupervisory committee: Linda Aguilar MA, David MacBryde BA, Dr. Matthias Manrique
Office & postal address:
Phone: +49 (0)30 612 808-72
Global2015 e. V.
Fax: +49 (0)30 612 808-74
Rungestrasse 22-24
10179 Berlin, Germany
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS, 8-10 June 2011
Berlin, June 2011Authors: Tammy L. Korndoerfer M.Sc., Dipl.-Pol. Lars Vogelsang, Zoe E. Richards, Gretchen Greywall MAContributors: Linda Aguilar BA, Sophie Bell BA, Denise Weiping Chak BA, Emma Nthandose Gausi B.Sc., Natalia Georgiadou M.Sc., Sarah Hartnett LL.B.(Ling.Germ.), Petr Novák LL.M., Madeleine Povey, Greg Stevenson B.Sc.(Hons), Jeanne-Marié Strauss MA, Kathryn M. Werntz, Ph.D. pre-candidatePhotographs: Tammy Korndoerfer Extended version
Special Global Challenges Report 1
Copyright Global2015 e. V.
Terms and condition
This report is available online
Printed on 100% recycled paper, chlorine-free, certified with the eco-label "Blue Angel" and the "EU Ecolabel" ("EU flower") , also complying to ISO 9706
and 14001. Binding comb is for postage purposes made of polypropylene, free of PVC and chlorine, easily recyclable.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
Table of ContentsSummary of UN Meeting Results 3
Countdown to Zero – Global Plan Towards the Elimination of New HIV Infections among Children by 2015 and Keeping their Mothers Alive 4
Introduction 5Section 1: The HIV/AIDS Epidemic 5
1.1 People Affected by HIV/AIDS 51.2 Deaths and Burden of Disease _ 71.3 Economic Damages _ 71.4 Human Rights 91.5 Goals _ 91.6 Targets _ 91.7 Trends _ 101.8 Recommended Measures and Internationally Agreed Upon Treatment and Prevention Targets _ 111.9 Costs and Benefits of Measures _ 16
Section 2: Interlinkages with Other Global Challenges 17
2.1 Poverty _ 182.2 Nutrition 192.3 Diseases and Co-infections _ 202.4 Safe Injections and Sterile Medical Equipment 212.5 Occupational Safety _ 222.6 Gender Equity _ 232.7 Safe Birthing Conditions _ 232.8 Access to Safe Water and Sanitary Living Conditions _ 252.9 Environment, Consumption of Natural Resources, and Land Usage _ 252.10 Conflict, Human Rights, and International Security 262.11 Preparedness for Natural Disasters 28
Key Points _ 28Annex 29
Goals 29Targets _ 29Human Rights _ 29
List of FiguresFig. 1: HIV/AIDS and Interlinking Global Challenges _ 5Fig. 2: Proportions of 4 Major Transmission Paths _ 6Fig. 3: Annual Deaths due to Global Challenges 8Fig. 4: Deaths due to AIDS (1990-2009) 10Fig. 5: New HIV Infections (1990-2009) 10Fig. 6: HIV-infected People (1990-2009) 11Fig. 7: Blood Donations Screened for HIV _ 14Fig. 8: Number of People Receiving Antiretroviral Therapy in Low- and Middle-income Countries _ 15Fig. 9: Target Achievements on HIV/AIDS by 2009 16Fig. 10: Major Sources of Financing 17Fig. 11: FAO Food Price Index 2000-2011 _ 19Fig. 12: Overlaps between HIV and TB (incidence and deaths) _ 20
List of TablesTable 1: Countries with Highest Number of HIV-infected Inhabitants 6Table 2: Top 10 Donor Countries _ 17

HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
Summary of UN Meeting Results
On 10th June 2011, the United Nations General Assembly, at the High-Level Meeting on AIDS, unanimously adopted the "Political Declaration on HIV/AIDS: Intensifying our Efforts to Eliminate HIV/AIDS", inclu-ding the following new goals and targets (emphasis always added):
"to end the epidemic with renewed political will" (§ 49).
General Assembly adopting the declara-
tion, 10/6/11 (UN Photo/JC McIlwaine)
"working towards reducing sexual transmission of HIV by 50 per cent by 2015" (§ 62);
"working towards the elimination of mother-to-child transmission of HIV by 2015 and
substantially reducing AIDS-related maternal deaths" (§ 64);
"Ensuring that women of child-bearing age have access to HIV prevention-related services and
that pregnant women have access to antenatal care, information, counselling and other HIV services" (§ 59 l);
"working towards reducing transmission of HIV among people who inject drugs by 50 per cent
by 2015" (§ 63);
"Expanding access to essential commodities, particularly male and female condoms and sterile injecting equipment" (§ 59 d); "Significantly expanding and promoting voluntary and confiden-tial HIV testing and counselling" (§ 59 f); "Promoting medical male circumcision where HIV pre-valence is high and male circumcision rates are low" (§ 59 i);
"Deploying new biomedical interventions as soon as they are validated, including female-initia-
ted prevention methods such as microbicides, HIV treatment prophylaxis, earlier treatment as prevention, and an HIV vaccine" (§ 59 n).
Universal access to treatment:
"redouble efforts to achieve, by 2015, universal access to HIV prevention, treatment, care
and support" (§ 51);
"accelerate efforts to achieve the goal of universal access to antiretroviral treatment . with the
target of working towards having 15 million people living with HIV on antiretroviral
treatment by 2015" (§ 66);
"combat tuberculosis, which is a leading cause of death among people living with HIV, . and
commit by 2015 to work towards reducing tuberculosis deaths in people living with
HIV by 50 per cent" (§ 75);
"reduce the high rates of HIV and hepatitis B and C co-infection" (§ 76).
"working towards closing the global HIV and AIDS resource gap by 2015, currently esti-
mated by the Joint United Nations Programme on HIV/AIDS to be $6 billion annually" (§ 86);
"Commit by 2015, through a series of incremental steps and through our shared responsibility,
to reach a significant level of annual global expenditure on HIV and AIDS, while re-
cognizing that the overall target estimated by the Joint United Nations Programme on HIV/
AIDS is between $22 billion and $24 billion in low- and middle-income countries" (§ 88).
The declaration also includes interlinkages between HIV/AIDS and poverty (§§ 7, 98), nutrition (§§ 70,
98), co-infections such as tuberculosis, hepatitis and malaria (§§ 69, 75, 76, 98-100), gender (§ 53), maternal and child health (§§ 98, 99), safe drinking water and sanitation (§ 98), and human rights (§ 77). However, topics such as the safety of medical injections and blood products are not covered.
UN 2011, General Assembly: Political Declaration on HIV/AIDS: Intensifying our Efforts to Eliminate HIV/AIDS. A/RES/65/277

HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
Countdown to Zero – Global Plan Towards the Elimination of New HIV
Infections among Children by 2015 and Keeping their Mothers Alive
As a side-event of the UN High-Level Meeting, the Global Plan The 22 most affected countries:
was started, agreed upon by 35 countries and 42 organizations Angola, Botswana, Burundi, Cameroon,
and business companies. These include the 22 countries in which Chad, Côte d'Ivoire, Democratic Re-
pregnant women are most affected by HIV infections, the US and public of the Congo, Ethiopia, Ghana,
other industrialized countries, UNAIDS, the World Bank, the Bill & India, Kenya, Lesotho, Malawi, Mozam-
Melinda Gates Foundation, the Clinton Health Access Initiative, bique, Namibia, Nigeria, South Africa, Merck, Roche, and others. This initiative encompasses the fol- Swaziland, Uganda, United Republic of lowing overall goals and targets (emphasis always added):
Tanzania, Zambia and Zimbabwe
"To accelerate progress towards the elimination of new child infections by 2015 and keeping
their mothers alive" (p. 38);
"Reduce the number of new HIV infections among children by 90%" until 2015; and
"Reduce the number of AIDS-related maternal deaths by 50%" until 2015 (p. 7).
Additionally, there are targets relating to 2015 in four strategic areas of prevention and treatment:
1. "Reduce HIV incidence in women 15-49 (and 15-24) by 50%";
2. "Reduce unmet need for family planning among women living with HIV to zero";
3. "Reduce mother-to-child transmission of HIV to 5%";
"90% of mothers receive perinatal antiretroviral therapy or prophylaxis";
"90% of breastfeeding infant-mother pairs receive antiretroviral therapy or prophylaxis";
4. "Provide 90% of pregnant women in need of antiretroviral therapy for their own
health with life-long antiretroviral therapy" (p. 39).
The Global Plan covers all low- and middle-income countries, but gives priority to the 22 countries in which the estimated numbers of pregnant women infected with HIV are the highest (p. 3).
Launch of the Global Plan. From left to right: Babalwa Mbono, mothers2mothers (South-African NGO); Michel Sidibé, Executive
Director of UNAIDS; Bill Clinton, Former President of the United States; UN Secretary-General Ban Ki-moon; Goodluck Jonathan,
President of Nigeria; and Eric Goosby, of the United States, Global AIDS Coordinator (UN Photo/Paulo Filgueiras)
The Global Plan includes many milestones, interim targets, and activities to ensure accountability, to
share responsibility, and to raise funds. Regarding funding required for the 22 most affected countries,
"the shortfall is . about US$ 2.5 billion for the period 2011-2015" (p. 18).
Because the transmission from mother to child cannot always be prevented, the funding requirements
of the Global Plan include the treatment of infants living with HIV in their first year of life, which is a
particularly critical period (p. 18). After the infants' first year, and regarding the mother after breast-
feeding has ended, the needs of mothers and children for HIV prevention and treatment shall be met
by already existing programmes on HIV prevention and treatment (p. 7). The "funds for ongoing treat-
ment for mothers beyond the breastfeeding period, for fathers and for children living with HIV" would
be required, but they "are not included in this Global Plan and must be mobilized separately" (p. 19).
UNAIDS 2011: Countdown to Zero; Global Plan Towards the Elimination of New HIV Infections among Children by 2015 and
Keeping their Mothers Alive; 2011-2015. (ISBN: 978-92-9173-897-7) Geneva.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
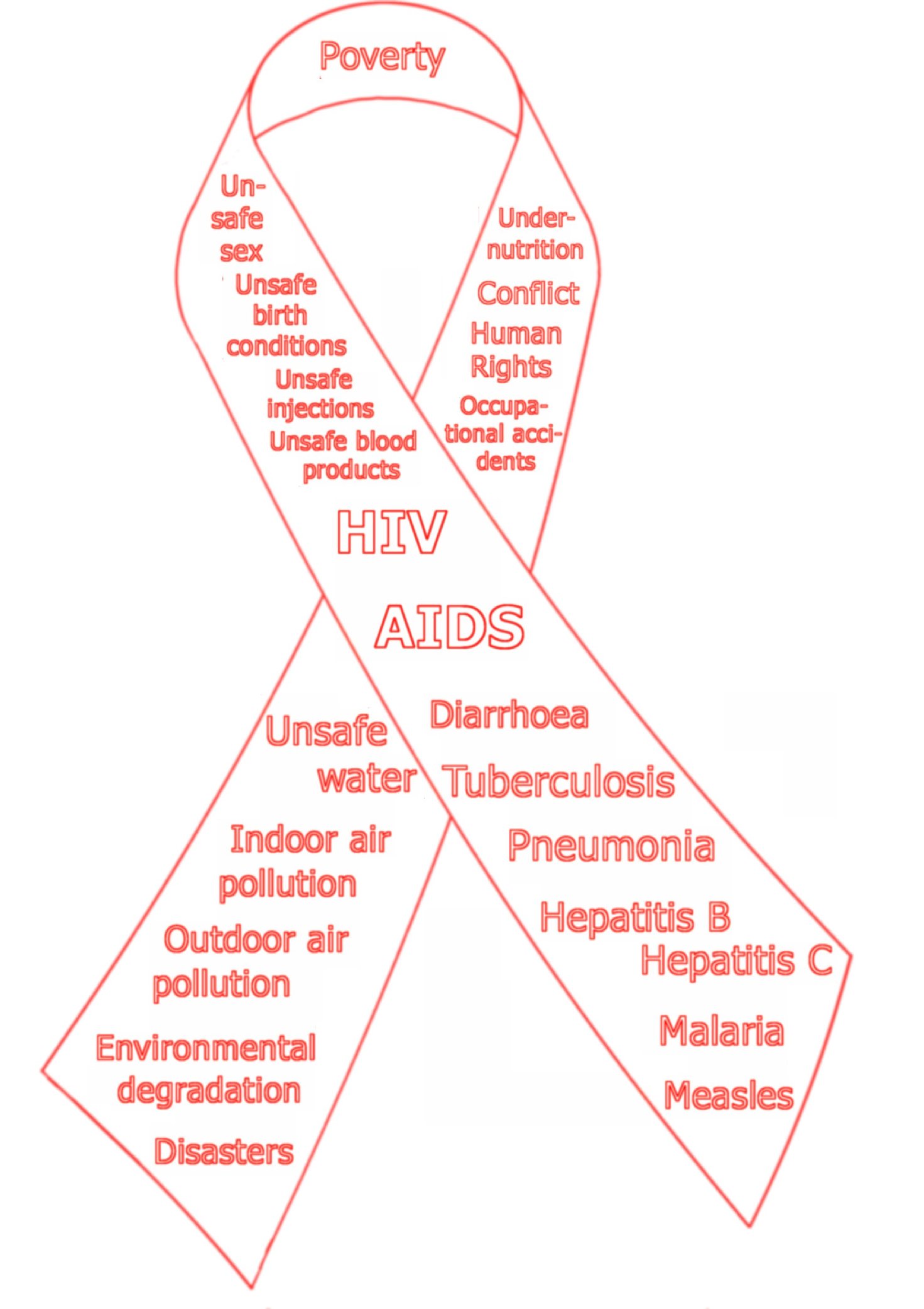
Human health worldwide is greatly affected by epidemics HIV/AIDS Basics
such as HIV/AIDS. The international community mobilized
an unprecedented level of financial resources, with 15.9 • The disease was first reported in
billion US dollars made available in 2009. However, an
1981 (AIDS, Acquired Immune
additional US$ 10 billion would have been necessary to
Deficiency Syndrome).
effectively fight HIV/AIDS globallyHIV/AIDS is, deservedly,
a well recognized and important global challenge. However, • The according virus was
like everything in a global context, it does not exist
discovered in 1983 (HIV, Human
independently from other global challenges. Almost every
major global challenge that the world is facing this century • 34 million people are infected.
has some connection to HIV/AIDS. It is beyond the scope of
this report to review them all; instead the focus is centred • 1.8 million deaths per year.
on some of the most relevant interlinkages between
HIV/AIDS and other global challenges. The fight against the • 58.5 million healthy life-years
epidemic can only be successful if interlinking factors do not
(DALYs) lost annually.
counteract and undermine the measures taken to tackle it.
This report may therefore be helpful in assessing strategies • US$ 52.3 billion, or 0.086% of
and setting priorities in the fight against HIV/AIDS.
global GDP in damages per year.
Fig. 1: HIV/AIDS and Interlinking Global Challenges
Section 1: The HIV/AIDS Epidemic
1.1 People Affected by HIV/AIDS
Cumulatively, up to 50.6 million people worldwide suffer from HIV/AIDS:
About 34 million people were living with HIV/AIDS in 2010 (estimates range from 30.9 to 36.9
million). That is 0.5% of the world population. Most of these (68%) live in sub-Saharan AfHIV/AIDS affects mostly people in the economically productive age range, reducing the work-force and, in doing so, constraining development. The most affected group among those living
UNAIDS 2010 – Joint United Nations Programme on HIV/AIDS: Global report; UNAIDS report on the global AIDS epidemic
2010. (ISBN 978-92-9173-871-7) Geneva.
p. 146.
UNAIDS 2011: AIDS at 30; Nations at the crossroads. Section 3
, p. 105; UNAIDS 2010 (fn. 1), pp. 23, 25, 180.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
with HIV is people aged 25-49 yRegarding new infections, young people aged 15-24 years account for 40% of all new
Table 1: Countries with
infections among adults
Highest Number of HIV-
Circa 16.6 million children have lost one or both parents to
infected Inhabitants
HIV can be transmitted by contact with infected blood or other body Nigeria
fluids, mainly through unprotected sexual intercourse, but also from mother to child (at birth or through breastfeeding), through unsafe India
injections in medical care, unsafe blood transfusions, and through sha-
red injection equip-
Fig. 2: Proportions of 4 Major Transmission Paths ment in injectable Tanzania
Sexual transmission (and injectable drug use, etc.)
HIV infections, about Uganda
14% were transmit-
Unsafe medical injections (range)
ted from mother to Zimbabwe
7% through unsafe Zambia
blood transfusions
Source: UNAIDS 2010 (fn. 1), pp.
Unsafe blood transfusions (range)
180, 187, 201.
an estimated 1.3% to 5%, and even up to 14% through unsafe injec-
Sources: UNAIDS 2010 (fn. 1), pp. 16, 19, 31, 78; AVERT
2011 (fn. 8); Walkley 2009 (fn. 8); WHO 2008 (fn. 9), p. 26; tions in health-care setRegarding transmis-
Hauri et al. [WHO] 2004 (fn. 6), p. 1834; SIGN/WHO,
sion through sharing injection equipment for drug
2011 (fn. 9), p. 4; own calculation.
use no global data is available; however, data on
UNAIDS 2010 (fn. 1), pp. 181, 183 (the global HIV prevalence among people 15-49 years is 0.8% [0.7-0.8%]; the prevalence
among young women 15-24 years is 0.6% [0.5-0.7%], and among young men 15-24 years 0.3% [0.2-0.3%] only; hence the prevalence among people 25-49 years is higher).
UN 2010, The Millenium Development Goals Report 2010. (ISBN 978-92-1-101218-7) New York. ,
UNAIDS 2010 (fn. 1), p. 186 (age: 0-17 years, uncertainty range: 14.4-18.8 million).
CDC 2010, Centers for Disease Control and Prevention: Basic Information about HIV and AIDS: How is HIV spread? August 11, 2010. ; WHO 2010, World Health Organization: HIV/AIDS; Online Q&A,
July 2010. WHO 2009, World Health Organization: Global Health Risks; Mortality and burden of disease attributable to selected major risks. (ISBN 978 92 4 156387 1) Geneva,
pp. 19, 22, 26; WHO 2002, World Health Organization: The World Health Report 2002, Reducing Risks, Promoting Healthy Life. (ISBN 1020-3311) Geneva.
pp. 62, 78-79; UNAIDS 2010 (fn. 1), pp. 19, 31; Reid, S., 2009, Non-vertical HIV transmission to children in sub-Saharan Africa, International Journal of STD & AIDS, (20) pp. 820-827; Reid, S.,
2009, Increase in clinical prevalence of AIDS implies increase in unsafe medical injections, International Journal of STD & AIDS (20), pp. 295-299; Hauri et al. [WHO] 2004, Comparative Quantification of Health Risks. Chapter 22: Contaminated
injections in health care settings, pp. 1803-1850 , p. 1831; Kane et al. 1999, Transmission of hepatitis B, hepatitis C and human immunodeficiency viruses through unsafe
injections in the developing world: model-based regional estimates, Bulletin of the World Health Organization, 1999, 77 (10), pp. 801-807 , p. 803; Lackritz, E.,
1998, Prevention of HIV transmission by blood transfusion in the developing world: achievements and continuing challenges, AIDS. 1998;12 Suppl A:S81-6.
Of 2.6 million new infections, there were 370 000 in children in 2009, which makes 14%; UNAIDS 2010 (fn. 1), pp. 16, 19,
78; own calculation.
WHO estimate: 5-10% of all new HIV cases in Africa; of all 2.6 million new infections, 1.8 million occur in sub-Saharan Africa;
hence it is 3.5-7% of all new infections; AVERT 2011: Blood Safety and HIV. (No date of publication given; according to meta data on last modification: 2011) Walkley, A., 2009: Africa: HIV Transmission Via
Transfusions in Continent Remains High own calculation.
WHO 2008, World Health Organization: The Global Burden of Disease; 2004 Update. (ISBN 978 92 4 156371 0)
, p. 26; Hauri et al. [WHO] 2004 (fn. 6), p. 1834; SIGN/WHO, 2011: Annual Meeting of the Safe Injection Global Network; 9 to 11 November 2010;
Dubai, United Arab Emirates , p. 4.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
Kenya (2006) show that about 3.8% of people newly infected with HIV were infected via this trans-mission Contracting other sexually transmitted diseases increases an individual's susceptibility to the HI virusIn most cases, if HIV is untreated for 7 to 10 years it progresses to AIDS, however this transition may occur more rapidly in less devSee also 2.4 on safe injections.
The global risk of HIV/AIDS is posed by possible changes in the patterns of spread, or changes in the
pathogen itself; this risk is characterized by a very large potential for damage as well as uncertainty
regarding the probability of occurrFor example, the frequency of antiretroviral resistant HIV in
high-income countries has already been observed increasing as a result of poor compliance with
antiretroviral therapy programmes
1.2 Deaths and Burden of Disease
In 2009, 1.8 million people died from DALYs: Disability-adjusted Life Years
HIV/AIDS related causesAIDS is the leading cause of death in Af(See figure One DALY represents the loss of one year of equi-3 on the next page, including data on other valent full health.
global challenges.)
DALYs are the sum of the years of life lost due to premature mortality (YLL) in the population and the
About 58.5 million healthy life-years years lost due to disability (YLD) for incident cases of
(DALYs) were lost due to HIV/AIDS in the health condition.
WHO, World Health Report 2004, p. 95.
1.3 Economic Damages
There is no comprehensive global data available, however:
In the United States of America, the cost of new HIV infections in 2002 was an estimated US$
36.4 billion, consisting of US$ 6.7 billion in direct medical costs and US$ 29.7 billion in
About US$ 15.9 billion was spent in 2009 to constrain HIV/AIDS, mainly in low and middle-
In countries that are highly affected by HIV/AIDS, the annual loss in GDP growth amounts to 2-
The losses expressed in dollars above amount to US$ 52.3 billion per year alone (this does not
include all economic costs).
10 UNAIDS 2010 (fn. 1), p. 31.
11 Bertozzi, S., et al. 2006: HIV/AIDS Prevention and Treatment. In: Disease Control Priorities in Developing Countries. 2nd
Edition. (ISBN 0-8213-0821361791) Washington DC, New York. , p. 335.
12 Ibid., p. 353; WHO 2010 (fn. 6).
13 WBGU 1998, German Advisory Council on Global Change (Wissenschaftlicher Beirat Globale Umweltveränderungen der Bun-
desregierung): World in Transition: Strategies for managing global environmental risks, Annual report 1998. Berlin, Heidel-
berg, New York, et al.: Springer, 2000 [publishing year of English version], pp. 62, 91.
14 Bertozzi et al. 2006 (fn. 11), p. 354.
15 Estimates range from 1.6 million to 2.1 million; UNAIDS 2010 (fn. 1), pp. 19, 21, 25.
16 UN 2010 (fn. 4), p. 40; WHO 2008 (fn. 9), pp. 54-58.
17 WHO 2008 (fn. 9), p. 60.
18 Discounted; Hutchinson, A. B., et al. 2006: The Economic Burden of HIV in the United States in the Era of Highly Active
Antiretroviral Therapy; Evidence of Continuing Racial and Ethnic Differences. In: Journal of Acquired Immune Deficiency
Syndromes, Volume 43, Number 4, December 1, 2006 , pp. 451.
19 UNAIDS 2010 (fn. 1), p. 146.
20 UN 2004, United Nations, Department of Economic and Social Affairs, Population division: The Impact of AIDS
, pp. 85, 89.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
Infectious diseases such as HIV/AIDS may shift to new regions and population segments. The per-ceived economic risk has been estimated by experts to likely cause an (additional) loss of about US$
250 billion within the next ten years (perceived probability of occurrence: 5-10%
Fig. 3: Annual Deaths due to Global Challenges
Undernutrition (under 5 years)
Indoor air pollution
Pneumonia (under 5 years)
Occupational diseases and accidents
Outdoor air pollution
Hepatitis B and C
Unsafe injections
Second-hand tobacco smoke
Natural disasters
Mid-range/ lower
Infectious diseases
The challenges included are mainly due to a lack of access to essential preconditions of life, such as food, health care and
physical integrity. – Data sources: undernutrition, indoor/outdoor air: WHO 2009 (fn. 6), pp. 13, 50; newborns: WHO 2008 (fn. 9), p. 54, UNICEF 2009: The State of The World's Children 2009, Maternal and Newborn Health, p. 2; unsafe water:
WHO/UNICEF 2010: Progress on Sanitation and Drinking-water, 2010 Update, p. 7; HIV/AIDS: UNAIDS 2010 (fn. 1), pp. 19, 21, 25; pneumonia: WHO, 2010, Pneumonia, Fact Sheet Number 331; occupational: WHO 2009 (fn. 6), p. 50, ILO 2009: World Day
for Safety and Health at Work 2009; Facts on safety and health at work, p. 1; TB, malaria, mothers: WHO 2011, World Health Statistics 2011, pp. 15, 16; roads: WHO 2009: Global status report on road safety, Time for Action, pp. 11, 1-3; hepatitis: Perz, J.
F., et al.: The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide, Journal of Hepatology 45 (2006), pp. 529-538, WHO 2010: Viral hepatitis, Report by the Secretariat (A63/15), §1, Wiersma, S.,
[WHO] 2010: Global Burden of Viral Hepatitis, pp. 10, 11; injections: WHO 2009 (fn. 6), p. 50, Miller, M. A., and Pisani, E.: The cost of unsafe injections, Bulletin of the World Health Organization, 1999, 77 (10), 808-811; smoke: WHO 2009: WHO Report on
the Global Tobacco Epidemic; Implementing smoke-free environments, p. 20; conflict: WHO 2008 (fn. 9), p. 58, WHO 2002 (fn. 6), p. 80, WHO 2004: World Health Report 2004, p. 124; measles: WHO/UNICEF 2010: Joint Annual Measles Report 2009;
Strengthening Immunization Services through Measles Control, p. 2; disasters: IFRC 2010: World Disasters Report 2010, p. 171 (average 2000-2009).
21 WEF 2010 – World Economic Forum: Global Risks 2010; A Global Risk Network Report. (ISBN 92-95044-31-2) Geneva.
, 2, pp. 44-45.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
1.4 Human Rights
The "right of everyone to the enjoyment of the highest attainable standard of physical and mental health" also applies to HIV/AIDS, regarding "the areas of prevention, treatment, care and support", and "addressing stigma and discrimination".
The international human rights system explicitly recognizes HIV status as a prohibited ground of discrimination.
Sources: resolution UN 2006 (fn. 65, General Assembly); resolution UN 2004 (fn. 195); UN 1976 (fn. 194), art. 12; UN 1948 (fn. 193); WHO 1946 (fn. 192); see quotes in the annex; UNHCHR/UNAIDS 2006 – Office of the United Nations High
Commissioner for Human Rights and the Joint United Nations Programme on HIV/AIDS: International Guidelines on HIV/AIDS and Human Rights; 2006 Consolidated Version.
1.5 Goals
1.6 Targets
The following goals have been agreed upon
The following internationally agreed upon,
time-bound, quantifiable targets have been
1. "to provide education and services to
prevent the transmission of all forms
1. with regard to 2015: "To have, by
of sexually transmitted diseases and
then, halted, and begun to re-
HIV and . improve care and support
verse, the spread of HIV/AIDS"
for people living with HIV/AIDS";
(Millennium Target);
2. "addressing the rising rates of HIV
2. "ensuring that . by 2010 prevalence
infection among young people to en-
. is reduced globally by 25 per cent"
sure an HIV-free future generation";
in persons 15 to 24 years of age
3. "To encourage the pharmaceutical
(UNGASS target [United Nations Gene-
industry to make essential drugs more
ral Assembly Special Session on
widely available and affordable by all
HIV/AIDS, 2001]);
who need them in developing coun-
3. "reduce the proportion of infants
tries" (Millennium Goal). Essential me-
infected with HIV . by 50 per cent by
dicines include antiretroviral drugs
2010" (UNGASS target).
against HIV/AIDS.
For targets on treatment please refer to the measures section below (1.8).
Sources: 1. UN 1999 (fn. 34, General Assembly), § 67,
Sources: 1. resolution UN 2000, General Assembly:
emphasis added; 2. resolution UN 2006 (fn. 65, General
United Nations Millennium Declaration
Assembly), § 26, emphasis added (see annex for full
quote and further goals); 3. resolution UN 2000, General
, § 19.4, emphasis added; 2. UN 1999 (fn. 34, General
Assembly: United Nations Millennium Declaration
Assembly), § 70, emphasis added [see annex for full
quote]; resolutions UN 2001 (fn. 34, General Assembly),
, § 20 [3], emphasis added; WHO 2010: WHO Model List
§ 47, and UN 2002 (fn. 34, General Assembly), § 46; 3.
of Essential Medicines; 16th list (updated). March 2010.
resolutions UN 2001 (fn. 34, General Assembly), § 54,
emphasis added [see annex for full quote], and UN 2002
(fn. 34, General Assembly), § 46.
In May 2011, the member states of the World Health Organization endorsed unanimously a strategy to fight HIV/AIDS, which includes the following targets:
by 2015, to "reduce HIV-related deaths by 25% (compared with a 2009 baseline)";
by 2015, to "reduce by 50% the percentage of young people aged 15–24 years who are
infected (compared with a 2009 baseline)";
and, by 2015, to "reduce new HIV infections in children by 90% (compared with a 2009
Source: WHO 2011 (fn. 59), § 22, emphasis added; resolution WHO 2011 (fn. 118).
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
1.7 Trends
+ / − The numbers of annual deaths and new infections are declining, however the number of
people reported to be living with HIV/AIDS is still rising.
+
The number of annual AIDS-related deaths is steadily decreasing from its peak of 2.1 million in
2004 to about 1.8 million in 2009Assuming that coverage with antiretroviral drugs continues to rise
at current rates, deaths worldwide from HIV/AIDS are expected to decline to 1.2 million in However, in 2009 the financial and economic crisis has flattened the funding of efforts to fight HIV/AIDS
Fig. 4: Deaths due to AIDS (1990-2009)
Source: UNAIDS 2010 (fn. 1), p. 24.
The number of people newly infected with HIV peaked in 1997 at 3.2 million, and has since declined to
2.6 million in Regarding new infections, the Millennium Target to halt, and to begin to reverse the spread of HIV/AIDS, has already been achieved at the global levOn the corresponding UN MDG indicator (the HIV prevalence among the population aged 15-24 years) there is no comprehensive data available (see belo
Fig. 5: New HIV Infections (1990-2009)
Source: UNAIDS 2010 (fn. 1), p. 16.
Another positive decline is found in the number of children who contracted HIV during the perinatal
and breastfeeding period – this number decreased from 500 000 in 2001 to about 370 000 in This is a reduction of 26% from 2001 to 2009. Unfortunately this is just over half the UN target of a
22 Uncertainty ranges: 1.9 million–2.3 million in 2004, 1.6 million–2.1 million in 2009, UNAIDS 2010 (fn. 1), pp. 19, 185.
23 WHO 2008 (fn. 9), pp. 22, 117, and WHO 2008a – World Health Organization: World Health Statistics 2008. (ISBN 978 92 4
0682740) Geneva. , p. 29.
24 UNAIDS 2010 (fn. 1), pp. 96, 146.
25 Uncertainty ranges: 3.0 million-3.5 million in 1997, 2.3-2.8 million in 2009, revised data; UNAIDS 2010 (fn. 1), pp. 16, 21,
184; UNAIDS 2011 (fn. 2), p. 99.
26 UNAIDS 2010 (fn. 1), p. 7; UN 2010 (fn. 4), p. 40.
27 UN 2010a – United Nations: The Millennium Development Goals Report 2010. [Statistical Annex]
, indicator 6.1; UN 2010b – United Nations: Report of the Secretary-General on the work of the Organization. (A/65/1, General Assembly, Official Records, Sixty-fifth
Session, Supplement No. 1.) (ISSN 0082-8173) New York. pp. 54-55.
28 Uncertainty ranges: 320 000–670 000 in 2001, 230 000–510 000 in 2009; UNAIDS 2010 (fn. 1), pp. 19, 78.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
50% reduction of infections among infants by 2010One of the primary barriers to further reductions in mother-to-child transmission is inadequate access to antenatal and postnatal servi(see also sub-section 2.7 on safe birth conditions in this report).
There is no comprehensive data available regarding the UN target to reduce the occurrence of HIV infections among young people aged 15-24 years by 25%, but in 15 of the worst affected countries
occurrence has fallen by more than 25% as young people have adopted safer sexual pr
The increase of people infected by HIV/AIDS has slowed as a result of intense efforts, but it has
still not been halted or reversed. The number of people living with HIV/AIDS has risen from 26.2 million in 1999 to 34 million in
Fig. 6: HIV-infected People (1990-2009)
Source: UNAIDS 2010 (fn. 1), p. 24.
Furthermore, the number of children who lost one or two parents due to HIV has increased from 14.6 million in 2005 to 16.6 million in
1.8 Recommended Measures and Internationally Agreed Upon Treatment
and Prevention Targets
Measures include preventing infection by information and education, access to testing and means of
protection, safe injections and safe blood transfusions; treatment of infection with antiretroviral
therapy (also for preventing mother-to-child transmission), avoiding stigmatization, and improving
conditions for resilience:
Preventing new infections:
Providing comprehensive and accurate knowledge about the transmission of
HIV and access to prevention: The UN members target to "ensure that . by 2010 at
least 95 per cent . of young men and women aged 15 to 24 have access to the
information, education and services" necessary to avoid HIV infAccording to
surveys, the global percentage of young men and women with this knowledge has
increased slightly – but at 34% it is far below the target level of 95% "Services should include access to preventive methods such as female and male
condoms, voluntary testing, counselling and follow-up"
29 Own calculation, based on abovementioned data.
30 UNAIDS 2010 (fn. 1), p. 64.
31 Ibid., p. 9.
32 Uncertainty ranges: 24.6 million–27.8 million in 1999, 30.9 million–36.9 million in 2010, revised data; UNAIDS 2010 (fn. 1), p.
23; UNAIDS 2011 (fn. 2), p. 65.
33 Uncertainty ranges: 12.4 million–17.1 million in 2005, 14.4 million–18.8 million in 2009, UNAIDS 2010 (fn. 1), p. 112.
34 UN 1999 – United Nations, General Assembly: Report of the Ad Hoc Committee of the Whole, Key actions for the further
implementation of the Programme of Action of the International Conference on Population and Development. (A/S-
21/5/Add.1) , § 70 [see annex for full quote]; resolution UN 2001, General Assembly: Declaration of Commitment on HIV/AIDS. § 47;
resolution UN 2002, General Assembly: A world fit for children. , § 46.
35 UNAIDS 2010 (fn. 1), p. 68; UN 2010 (fn. 4), p. 41.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
o Only consistent abstinence provides a 100% prevention of sexually transmitted
HIVHowever, campaigns limited to abstinence showed little effect on sexual beha
o The risk of infection increases with the number of sexo Choosing a partner who tested HIV-negative instead of an untested partner reduces
the relative risk of HIV infection 47-fold (or by Living in a mutually monogamous relationship combined with undergoing regular retesting is also an effective risk-reduction strategy
o Treating HIV-infected people with antiretroviral therapy (ARVT) is also a very
effective prevention measure. According to very recent research, ARVT reduces the rate of transmission to an uninfected partner by 96%
o The use of condoms provides the highest degree of HIV infection prevention
available from devices. Consistently using male latex condoms provides 80-95% fewer infections than never using them during interComprehensive prevention campaigns led to safer sexual behaviours and fewer HIV inf
o Without replacing other known methods of HIV prevention, adult male circumcision
is recommended in areas of high HIV prevalence as it is associated with a lower risk of HIV infection (55-76% relative risk reduction) for men – partial, but lif
o Further factors influencing to different degrees the transmission of HIV include the
duration of sexual relationships, the frequency of partner change, multiple partner-ships, early or late sexual debut, sex between people of different generations, types of sexual intercourse, and other related issues
36 UN 1999 (fn. 34), § 70, emphasis added [see the annex for full quote]; resolution UN 2001 (fn. 34), § 47; resolution UN 2002
(fn. 34), § 46.
37 WHO 2010 (fn. 6).
38 Bertozzi et al. 2006 (fn. 11), p. 344, 337; Bennett, S. E., and Assefi, N. P., 2005, School-based teenage pregnancy prevention
programs: A systematic review of randomized controlled trials. In: Journal of Adolescent Health, Volume 36, Issue 1, pp. 72-81 p. 80.
39 Varghese et al. 2002: Reducing the Risk of Sexual HIV Transmission; Quantifying the Per-Act Risk for HIV on the Basis of
Choice of Partner, Sex Act, and Condom Use. In: Sexually Transmitted Diseases, 9(1):38-43.
, pp. 41-42.
40 Ibid, pp. 39-41; own calculation.
41 Ibid, p. 42.
42 WHO 2011: Groundbreaking trial results confirm HIV treatment prevents transmission of HIV.
National Institute of Allergy and Infectious Diseases (NIAID) 2011: Treating HIV-infected People with Antiretrovirals Protects Partners from Infection; Findings Result from NIH-
funded International Study
43 World Health Organization, Johns Hopkins Bloomberg School of Public Health and United States Agency for International
Development, 2008: Family Planning; A Global Handbook for Providers; Evidence-based guidance developed through worldwide collaboration. (2008 Update.) (ISBN 978-0-9788563-0-4) Baltimore and Geneva, p. 192; Varghese et al. 2002 (fn.
39), p. 40; NIAID 2001 – National Institute of Allergy and Infectious Diseases: Workshop Summary: Scientific Evidence on Condom Effectiveness for Sexually Transmitted Disease (STD) Prevention; June 12-13, 2000; Hyatt Dulles Airport. Herndon.
pp. 7-8, 14.
44 Bertozzi et al. 2006 (fn. 11), pp. 344, 337-338.
45 UNAIDS 2010 (fn. 1), 81; WHO et al. 2010 – World Health Organization, UNAIDS and UNICEF: Towards universal access;
Scaling up priority HIV/AIDS interventions in the health sector; Progress report 2010.
p. 37; WHO 2010 (fn. 6); CDC 2008 – Centers for Disease Control and Prevention: Male Circumcision and Risk for HIV Transmission and Other Health Conditions: Implications
for the United States. Updated February 2008. , p. 2; UNAIDS 2011: AIDS at 30; Nations at the crossroads. Sub-section 1.9
46 Mah, T. L., and Halperin, D. T., 2008: Concurrent Sexual Partnerships and the HIV Epidemics in Africa: Evidence to Move
Forward. In: AIDS and Behavior, Volume 14, Number 1, 11-16.
Lurie, M. N., and Rosenthal, S., 2008: Concurrent Partnerships as a Driver of the HIV Epidemic in Sub-Saharan Africa? The Evidence is Limited. In: AIDS and Behavior, Volume 14, Number 1, 17-24.
Hertog, S., 2007: Heterosexual behavior patterns and the spread of HIV/AIDS: the interacting effects of rate of partner change and sexual mixing. In: Sexually Transmitted Diseases
Volume 34, Number 10, 820-8
Prevention programmes shall include most or all of the available strategies and means of prevention, including public educationInformation should also cover how to prevent other transmission paths, including from mother to child and through unsafe injections and blood transfusions (see below). Voluntary testing and counselling should be available for couples, in particular. In 36-85% of couples in 12 sub-Saharan countries one partner is HIV-infected and the other one is HIV-negativMost new infections happen to people in such couples. Voluntary testing and counselling motivates such couples to practice safer sexual behaviours more effectively than individual testing and counsellBy sharing knowledge of HIV status, couples are able to make plans and vital decisions together, and to seek joint care and suppo HIV prevention programmes should reach all groups largely involved in the spread of HIV (young men and women, sex workers and their clients, men who have sex with men, and people who inject drugs)Effectiveness of HIV prevention programmes is increased by peer approaches, involving faith-based groups and leaders, empowering women and girls, and providing screening and treatment of other sexually transmitted y of the preventive measures mentioned also help to avoid infections with other sexually transmitted diseases, such as hepatitis B.
Preventing transmission from mother to child by voluntary testing, pro-
phylactic treatment and expanded access to maternal and infant health
services: The proportion of pregnant women in low- and middle-income countries who
received an HIV test reached 26% in 2009, showing an increase from 7% in 2005More than 60% of pregnant women who were confirmed HIV positive in low- and
middle-income countries received antiretroviral medication to prevent the mother-to-
child transmission in 2010, in comparison to 15% in 2005Antiretroviral prophylaxis is
recommended during pregnancy, delivery, and also during breastfeeding. An alternative
or additional method to reduce the transmission risk during delivery is caesarean section
(see 2.7 on safe birth conditions).
Regarding breastfeeding, in less developed regions where access to safe water is
lacking and child-killing diseases are common, breastfeeding combined with antiretro-
viral prophylaxis minimizes the risk of HIV transmission and maximizes the child's chance
of survival regarding other fatal diseases, because of the natural immunity provided by
breast Where antiretroviral prophylaxis is not provided, babies should be given
Hallett, T. B., et al. 2007: Behaviour change in generalized HIV epidemics: impact of reducing
cross-generational sex and delaying age at sexual debut. In: Sexually Transmitted Infections Volume 83:i50-i54. Garnett, G. P., 1998: The Basic Reproductive Rate of Infection and the
Course of HIV Epidemics. In: AIDS Patient Care and STDs. Volume 12 Number 6, 435-449. Le Pont, F., and Valleron, A. J., 1991: Impact of temporal
patterns of sex partner change on the HIV epidemic in an heterosexual population. In: International Conference on AIDS. Jun 16-21, 1991; 7: 411.
47 UNAIDS 2010 (fn. 1), 85.
48 UNAIDS 2010 (fn. 1), 30.
49 Kennedy, C. E., et al., 2010: Behavioural interventions for HIV positive prevention in developing countries; A systematic review
and meta-analysis. In: Bulletin of the World Health Organization 88: 615-623.
50 WHO 2011: HIV testing and counselling. (No year of publication given; according to metadata: publishing year 2011.)
51 UNAIDS 2010 (fn. 1), 85.
52 Bertozzi et al. 2006 (fn. 11), pp. 348-349.
53 WHO et al. 2010 (fn. 45), 86; UNAIDS 2010 (fn. 1), p. 78.
54 UNAIDS 2011: AIDS at 30; Nations at the crossroads. Sub-section 1.11
, p. 72; WHO et al. 2010 (fn. 45), 83; UNAIDS 2010 (fn. 1), p. 78.
55 WHO et al. 2010 – WHO, UNAIDS, UNFPA and UNICEF: Guidelines on HIV and infant feeding 2010; Principles and
recommendations for infant feeding in the context of HIV and a summary of evidence. (ISBN 978 92 4 159953 5) pp. 35, 37-38; UNAIDS 2010 (fn. 1), p. 79; Kesho
Bora 2011, Triple antiretroviral compared with zidovudine and single-dose nevirapine prophylaxis during pregnancy and breastfeeding for prevention of mother-to-child transmission of HIV-1 (Kesho Bora study): a randomised controlled trial. In:
The Lancet Infectious Diseases, Early Online Publication, 14 January 2011. pp. 6-8; WHO 2011 (fn. 42), p. 2.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
infant formula prepared using safe water, or heat-treated breast miNevertheless, as long as sufficient access to safe water and child health care are not provided, mothers are presented with a difficult choice between two life-threatening options. Maternal and child health services must be further strengthened to reduce mother-to-child trans-– see sub-section 2.7 on safe birth conditions. Continuing antiretroviral treat-ment of HIV infected mothers reduces the risk of increased drug resistance of HIV, as well as the number of children orphaned in the futur
Ensuring injection safety through sustainable procurement of sufficient
quantities of appropriate syringes, avoiding unnecessary injections, informing
about the risks of injections, training in safe injection practices, and ensuring
that sharps waste (e. g. used needles and scalpals) is properly manage–
see sub-section 2.4 on safe injections.
En onations
suring Screened f
blood s or HIV
afety by introducing Scr
eff eened
ective blood donor Not screened
selection and
quality-assured screening of all donated blood and blood products, as well as
training clinicians and nurses in safe clinical transfusion practices (including
High-income acountries
ppropriate use of blood in order to minimize unnecessary tr 99.50%
ansfusions, and informing 0.50%
about the risks of transfusions
Blood safety is already improving,
Fig. 7: Blood Donations Screened for HIV
Low-income countries
but as of 2009, 38 of the 165
countries participating in a survey 100%
still reported that they have not screened all or even any blood donations for HIV in a quality-
assured mannerGlobally, however,
about 93.1% of blood donations were screened for HIV in a quality-assured manner during the period of
2007-09: in high-income countries
99.5%, in middle-income-countries
countries countries countries
85.4%, and in low-income countries 47.8%These measures, as well as
Data source: WHO et al. 2010 (fn. 45), p. 43.
providing injection safety, also help to prevent infections with other blood-borne diseases, such as hepatitis B and C.
"Expanded access . to sterile injecting equipment" by e. g. through
needle or syringe exchange programmes for injectable drug users. Other harm reduction measures, such as ready access to effective drug treatment and substitution, and provision of counselling and condoms, can also help to reduce the spread of HIV/AIDS
Providing antiretroviral therapy and care, for "coming as close as possible to the
goal of universal access to treatment by 2010 for all those who need it"About 6.6
million people in low- and middle-income countries were accessing antiretroviral drugs at the end of 2010, up from around 4.05 million in 2008. The coverage of antiretroviral treatment in
56 WHO et al. 2010 (fn. 55), pp. 35, 37-38.
57 UNAIDS 2010 (fn. 1), pp. 115, 9, 64.
58 Kesho Bora 2011 (fn. 55), p. 8; Bertozzi et al. 2006 (fn. 11), p. 345; UNAIDS 2010 (fn. 1), p. 155.
59 Resolution UN 2001 (fn. 34), § 51; WHO 2011: Draft WHO HIV strategy 2011–2015; Report by the Secretariat. (A64/15)
, § 36; WHO 2002 (fn. 6), pp. 130-131; Hauri et al. [WHO]
2004 (fn. 6), p. 1840; Reid, 2009 (fn. 6), p. 298.
60 WHO 2005, 58th World Health Assembly: Blood safety: proposal to establish World Blood Donor Day. (Resolution WHA58.13)
§3 [7] e, f; WHO 2011 (fn. 59), §§ 36 and 75.
61 Summary of table from UNAIDS 2010 (fn. 1), pp. 245-247, 217.
62 WHO et al. 2010 (fn. 45), p. 43.
63 Resolution UN 2001 (fn. 34), § 52.
64 Bertozzi et al. 2006 (fn. 11), p. 346.
65 Resolution UN 2006 – United Nations, General Assembly: Political Declaration on HIV/AIDS. (A/RES/60/262)
§ 57 d, emphasis added.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
low- and middle-income countries increased 22-
Fig. 8: Number of People Receiving
fold since Despite limited availability,
Antiretroviral Therapy in Low- and Middle-
approximately 2.9 million deaths have been
income Countries, 2002–2009 (Millions)
averted because of antiretroviral dFur-thermore, antiretroviral therapy reduces the infectiousness of treated individuals, and the availability of treatment destigmatizes the di-sease and increases the effectiveness of preven-tion progrAlthough substantial, these achievements are far removed from the target of universal access: about 36% of the 14.6 million people in need in low- and middle-income countries were receiving antiretroviral therapy in 2009; where globally more than 9 million people
Source: WHO et al. 2010 (fn. 45), p. 53.
still remain in need of treatment There is also a lack of treatment for opportunistic diseases (such as tuberculosis), as well as a lack of palliative and home-based care, including pain managemeMalnutrition, which impairs treatment, is addressed through counselling, daily micronutrient supplements, food rations, therapeutic food, school feeding with take-home rations for families caring for orphans, food for training and food for work programmes
Research and development on improved treatment, vaccines and other preventive
methods: A preventive vaginal microbicide gel (28-54% relative risk reduction for women) will
be introduced following further testingOngoing trials on the preventive use of antiretroviral
drugs before exposure to HIV, as well as the development of vaccines, may provide major
improvements in the fight against HIV/AINew research showed that using a persistent
virus as a vaccine vector enables immune cells of monkeys to clear SIV from the body (SIV is
the equivalent of HIV in monkeys, and the most likely origin
Protecting human rights of all people affected by HIV is a precept and makes
prevention efforts more effective. The human rights of key populations at higher risk of
exposure to HIV, such as prostitutes, men who have sex with men, and injectable drug users,
should be recognized and addressed. National programmes to reduce HIV-related stigma and
discrimination should be in place and better implemented. Addressing discrimination avoids
driving HIV underground, inhibits transmission pathways, and helps to expand access to life-
saving HIV prevention, treatment, care and suppoSee also 2.10 on human rights issues.
Including structural activities into prevention can reduce the numbers of new HIV
infections: providing food security and microfinance for women, schooling or cash transfers for
girls, and crisis response services to street-based sex worke
66 UNAIDS 2011: AIDS at 30; Nations at the crossroads. Sub-section 1.1
, p. 42; WHO et al. 2010 (fn. 45), pp. 51-54; UNAIDS 2010 (fn. 1), pp. 96, 8.
67 UN 2010 (fn. 4), p. 45.
68 Bertozzi et al. 2006 (fn. 11), p. 349; A Castro and P Farmer 2005: Understanding and Addressing AIDS-Related Stigma: From
Anthropological Theory to Clinical Practice in Haiti. In: American Journal of Public Health 95 (1): pp. 53-59, p. 56.
69 Revised data; WHO et al. 2010 (fn. 45), pp. 53, 55; UNAIDS 2010 (fn. 1), p. 8; own calculation; UNAIDS 2011 (fn. 66), p. 43.
70 UNAIDS 2010 (fn. 1), p. 109; Bertozzi et al. 2006 (fn. 11), pp. 351-352.
71 Bertozzi et al. 2006 (fn. 11), pp. 352-353.
72 UNAIDS 2010 (fn. 1), p. 83; WHO et al. 2010 (fn. 45), p. 43; Abdool Karim, Q., et al., 2010, Effectiveness and Safety of
Tenofovir Gel, an Antiretroviral Microbicide, for the Prevention of HIV Infection in Women, Science, Vol. 329, no. 5996,
, pp. 1168-1174.
73 WHO et al. 2010 (fn. 45), pp. 25, 43; UNAIDS 2008, Report on the global HIV/AIDS epidemic 2008, ISBN 978 92 9 173711 6,
Geneva, p. 106. RM Grant, et al.: Preexposure Chemoprophylaxis for HIV Prevention in Men Who Have Sex with Men. In: The New England Journal of Medicine,
74 Hansen, S. G., et al. 2011: Profound early control of highly pathogenic SIV by an effector memory T-cell vaccine. In: Nature,
Volume 473, 523–527
75 WHO et al. 2010 (fn. 45), p. 106; UNAIDS 2010 (fn. 1), pp. 8, 121, 137.
76 UNAIDS 2010 (fn. 1), pp. 76.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
Fig. 9: Target Achievements on HIV/AIDS by 2009
Halt and begin to
reverse the spread by
Halve infections
among infants by 2010
Access to information
for 95% of young
Universal access to
treatment by 2010
Target achievement
Gap to target level
Target achievement
Data sources: UNAIDS 2010 (fn. 1), p. 7; UNAIDS 2010 (fn. 1), pp. 19, 78; UNAIDS 2010
(fn. 1), p. 68; WHO et al. 2010 (fn. 45), pp. 53, 55; own calculations of percentages. Global2015
1.9 Costs and Benefits of Measures
About US$ 15.9 billion were available in 2009 to constrain HIV/AIDS, mainly in low and middle-income
countries. However, this still left a US$ 10 billion funding gapIn 2010 at least US$ 26.7 billion
(0.044% of gross world product) would have been needed to meet the 2010 target of universal access
to prevention and treatmentThe costs to achieve safe and appropriate use of injections in
transitional and developing countries were estimated to be US$ 905 million in The G8 has
pledged "to work towards the goals of providing at least a projected US$ 60 billion over 5 years, to
fight infectious diseases and strengthen health"In economic terms, benefits of the main measures to fight HIV/AIDS are 1 to 12 times as high as their
Major Sources of Financing
costs. However, some measures are even more cost-effective. To avert 2 million new infections and to
healthy life- years (DALYs) by a combination of different prevention measures requires
an estimated US$ 2.5 billion per year, with benefits 12-times the costs (assuming the value of a 52%
to be more than double the annual per capita income in low-income countries, or US$ 1.000)By
including treatment, to avert 28 million new infections within 10 years requires US$ 122 billion 42%
that decade, but saves the higher costs of future treatmentCost-effectiveness of prevention
measur ropic sect
if the national or local prevalence of HIV is low.
Blood screening for HIV is costly but has been shown to be cost-effective, with median costs of US$ 11 (0.45-2,259) per DALY saved. Screening all blood for transfusions and providing sterile injections is recommended as being cost-effective even in a low-level In less developed countries, voluntary counselling and testing costs a median US$ 19 (10-261) per saved DALY, but depends strongly on HIV prevalence and is hence cost-effective only for risk groups, or in a high-level epidemic areHowever, there may be other good reasons to offer testing, e. g. to enable people to know their
77 Ibid., pp. 146.
78 WHO et al. 2010 (fn. 45), 10.
79 Dziekan, G., et al., 2003: The cost-effectiveness of policies for the safe and appropriate use of injection in healthcare settings,
Bulletin of the World Health Organization 81(4), pp. 277-285.
277; WHO 2004a, Safety of Injections, Global Facts & Figures. (WHO/EHT/04.04) , p. 2.
80 G8 2008, Group of Eight industrialized countries:
§ 46a; affirmed in G8 2009,
81 Jamison, D. T., P. Jha and D. Bloom, 2008: Disease Control. (Copenhagen Consensus 2008 Challenge Paper; Diseases)
October 2007, revised April 2008.
, pp. 51, 27.
82 Stover, J., et al. 2006: The Global Impact of Scaling Up HIV/AIDS Prevention Programs in Low- and Middle-Income Countries.
In: Science Magazine Vp. 1474.
83 Bertozzi et al. 2006 (fn. 11), pp. 346, 348, 342; median taken from reported values.
84 Ibid, pp. 339, 348-349; median taken from reported values.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
HIV status, or as an entry point to Fig. 10: Major Sources of Financing Table 2: Top 10 Donor
HIV prevention and carInjection-
Countries (Million US$ in
related infections could be reduced
at an average cost of US$ 102 per
DALY by applying a combined policy
strategy of single-use syringes and
Philanthropic United Kingdom
interventions to minimize injection Preventing mother-to-child
HIV transmission by antiretroviral
drugs costs a median US$ 126-154
Source: UNAIDS 2010 (fn. 1), p. 146;
WHO et al. 2010 (fn. 45), p. 10.
(6-2.303) per DALY sav Antiretroviral treatment is expensive, but the benefits are in many Denmark
instances larger than the cTo save a DALY through antiretroviral Sweden
drugs in less developed countries costed about US$ 350 in 2001 (first-line therThe median price of the most common adult first-line Spain
antiretrovirals continued to decrease in low-income, lower-middle income Japan
and upper-middle countries between 2008 and October 2010. The decrease in the observed price varied from 12% up to 77%The Norway
median price of second-line drugs, which are applied after resistance or Source: UNAIDS 2010 (fn. 1), pp. severe side effects of the first-line therapy have occurred, also decreased 150-151; Kates, J., et al., 2010,
Financing the response to AIDS
between 2008 and October 2010 but at a smaller magnitude. The most in low- and middle-income coun-
common second-line regimen prescribed for adults decreased in price by tries: international assistance
15% in low income countries, 62% in lower-middle income countries and from the G8, European Com-80% in upper middle-income cThe price of second-line regi- mission and other donor govern-mens continues to decrease but their cost remains 6 to 30 times higher ments in 2009. Geneva
than that of the least expensive first-line regimen
Section 2: Interlinkages with Other Global Challenges
"[W]e face a new generation of threats, unlike any in history, which spill across borders and have
global reach. No single country or group, however powerful, can deal with them alone. All must
work together – in common cause for common solutions – to address challenges like climate
change, poverty, and nuclear disarmament . Collective action has never been easy, but it has
never been more necessary than in achieving the UN's Millennium Development Goals – the world's
blueprint for ending extreme poverty. The conventional wisdom will tell you that the MDGs targets
– reducing poverty and hunger, improving the health of mothers and children, combating
HIV/AIDS, increasing access to education, protecting the environment, and forging a global
partnership for development – are simply unattainable. In fact, we are controlling disease – polio,
malaria, and AIDS – better than ever before, and making big new investments in women's and
children's health – the key to progress in many other areas."
Ban Ki-Moon, 2010, New Directions for the UN, United
85 WHO 2003: The right to know; New approaches to HIV testing and counselling. (WHO/HIV/2003.08)
86 Dziekan et al. 2003 (fn. 79), p. 277; WHO 2004a (fn. 79), p. 2, Bertozzi et al. 2006 (fn. 11), p. 346.
87 Bertozzi et al. 2006 (fn. 11), p. 341; upper and lower median taken from reported values.
88 Jamison et al. 2008 (fn. 81), p. 41.
89 Bertozzi et al. 2006 (fn. 11), p. 356.
90 WHO 2011, World Health Organization: Transaction prices for antiretroviral medicines and HIV diagnostics from 2008 to
October 2010; A summary report from the Global Price Reporting Mechanism. December 2010
91 Ibid., p. 9.
92 Ibid., p. 22.

HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
2.1 Poverty
Although the HI virus does not discriminate, and affects the wealthy as well as the under-privileged,
the most affected countries are among the poorest in the woThe rate of people living with HIV in
the least developed countries is nine times higher than the rate in more developed regionsMost
governments have prevention programmes in place, but in some cases these are less effective than
they could be with better information and funding, and many of the individuals most in need do not
have access to basic prevention programmes because of their impoverished sta Poverty contributes strongly to individuals partaking in behaviours that expose them to an increased
risk of infection. In most cases this is due to a lack of knowledge on how to prevent infection.Poverty
can also prevent those who have been infected from accessing the life-long care that HIV/AIDS
requires. Although it is generally believed that it is the rural and uneducated individuals that are more
likely to engage in high-risk sex and less likely to use condoms, due to being poorly infdata
has shown that it is usually the better-off members of society who have the highest HIV/AIDS
transmission rate in these less developed countries. It seems that HIV is transmitted mainly to urban,
employed, and more mobile members of these However, HIV/AIDS often increases the
burden of poverty where it already and pushes previously unimpoverished people into poverty
by placing heavy financial burdens on families and breaking down inter-generational suppor There are several poverty-related factors which increase exposure to HIV/AIDS. Financial constraints
influence occupational decisions (including participating in the sex trade) which carry a high risk of
participating in unprotected sex, and poverty has also been linked to a lowered fear of contracting
HIV/AIDSOne theory behind this is that impoverished people are generally less likely to be concerned with the future and are forced to be more concerned with day to day surviv Another reason that poverty is associated with a higher risk of contracting HIV/AIDS is family life. The WHO notes that poverty plays a pivotal role in teenage marriage, a factor that leads to the spread of sexually transmitted diseases including HIV (this can also be exacerbated by the practice of poly-gamy). Young girls often have no choice about having unprotected sex with their hus-bands and makes them vulnerable to con-tracting the HI virus from their infected hus-
Mambil a women working their farm in Nigeria
93 UN Department of Social and Economic Affairs, 2005, Population, Development and HIV/AIDS with Particular Emphasis on
Poverty: The Concise Reporp. 55.
94 Ibid., p. 55.
95 Ibid., p. 57.
96 Ibid., pp. 1-2.
97 Ibid., p. 30.
98 IFRC (International Federation of Red Cross and Red Crescent Societies), 2008, World Disasters Report 2008: Focus on HIV
and AIDS. , p. 34; Piot P, Greener R, Russell S
(2007): Squaring the circle: AIDS, poverty, and human development. PLoS Med 4(10): e314 (doi:10.1371/journal.pmed.0040314), p. 1571.
99 IFRC, 2008 (fn. 98), pp. 41, 42.
100 Ibid., p. 3.
101 Ibid., pp. 8, 34, 50.
102 SARPN Conference 2006, [in] Mbirimtengerenji, N., 2007, Croatian Medical Journal, (48) 5,
, pp. 605-617.
103 University of Illinois at Chicago, Conference Report on African Studies 2005: Teenage Marriages in Africa [in]
Mbirimtengerenji, N., 2007, Croatian Medical Journal, (48) , p. 145.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
2.2 Nutrition
In 2010, about 925 million people were undernourishedand undernutrition accelerates the
development of immune deficiency and opportunistic infIt can also increase the side effects
of antiviral therapyTwo thirds of HIV/AIDS sufferers live in Sub-Saharan Africa, where undernutrition
rates are high. Undernutrition can compound the complications and side effects of antiretroviral
therapy and other types of car Similarly HIV/AIDS also has a strong influence on undernutrion. Children who have been orphaned
due to HIV/AIDS (or are living with parents who are living with HIV and therefore unable to provide a
livelihood) are likely to be undernourished. An estimated 16.6 million children have lost either one or
both parents because of AIDS. Furthermore, food is likely to be scarce in areas highly affected by
HIV/AIDSIn times of nutritional emergency, further problems are generated, which include
disrupting education and a rise in sex-related crimes towards women and children. These situations can
contribute to the spread of HIV/AIDS Even when adequate nutrition is available, people in the advanced stages of AIDS will suffer
symptoms similar to those of undernutrition: weight loss, nutrient deficiencies, and wasting. This is due
to a combination of increased metabolic demand, loss of appetite, gastrointestinal malabsorption and
body redistribution.
A lack of vital nutrients in people living with HIV/AIDS is linked to a higher rate of mortality and HIV
progression. Nutrients can be supplemented with vitamin tablets, which can slow down the progression
of the virus even in those who are not undergoing antiretroviral therapyWhen affected with HIV,
regular bouts of illness often occur. These periods of sickness are likely to alter a patient's appetite as
well as increase the body's demand for nutri-
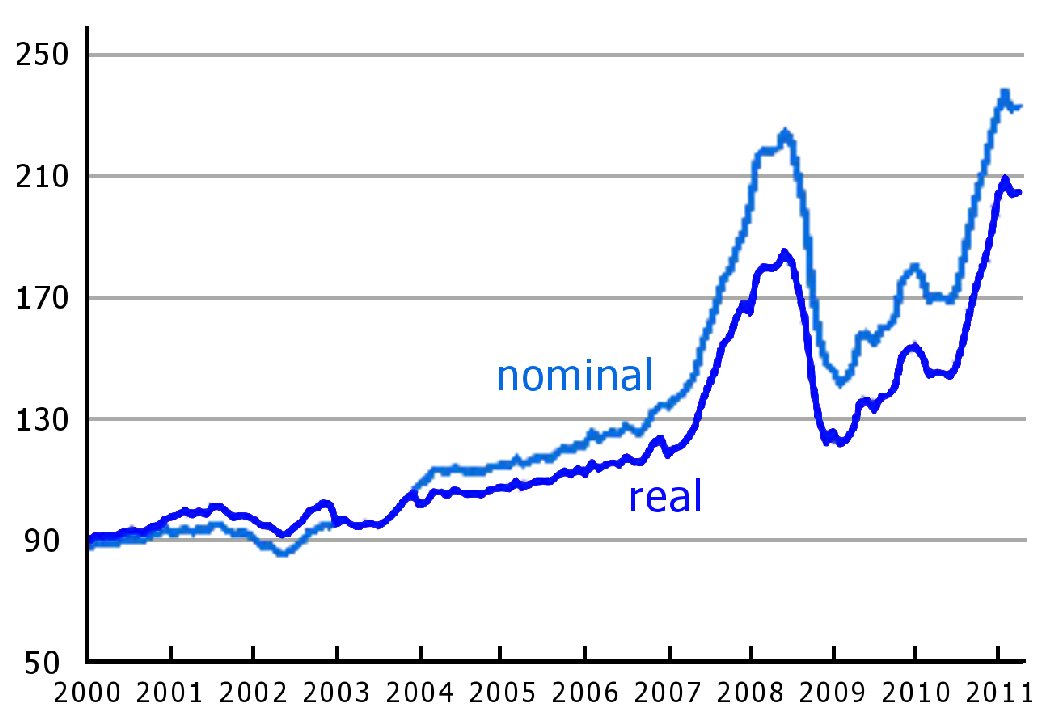
Fig. 11: FAO Food Price Index 2000-2011
Currently, the FAO Food Price Index shows that food prices are higher than they have ever been. Naturally, impoverished countries are largely affected by this increase and many people are not able to afford food. They are therefore likely to become undernourished, and this in turn will lead to a faster progression of HIV to AIDS A number of organizations, which focus on tackling HIV/AIDS and undernourishment, have been established. This integrated approach to fighting HIV/AIDS has had demonstrable success, assisted by support from the UN and other aFor example, UNICEF, along with the Department for International Development (DFID) have co-lead a number of programmes in 2002-2004=100. Source: FAO Food Price Index, 05/05/2011Sub-Saharan Africa, South-East Asia, and the
104 FAO, 2010, Addressing Food Insecurity in Protracted Crise.
105 IFRC, 2008 (fn. 98), p. 145.
106 Ivers, L., et. al., 2009, HIV/AIDS, Undernutrition and Food Insecurity, Clinical Infectious Diseases, 49,
p. 1097; Bertozzi et. al., 2006 (fn. 11), p. 352.
107 WHO, 2008, Regional Consultation on Nutrition and HIV/AIDS in French speaking countries,
108 UNAIDS 2010 (fn. 1), p. 186.; UNICEF, 2008, Nutrition and HIV/AIDS, .
109 UNICEF, 2008, HIV's high nutritional toll,
110 Drain, P. K., et al., 2007: Micronutrients in HIV-positive persons receiving highly active antiretroviral therapy. In: The American
Journal of Clinical Nutrition., p. 333.
111 FAO, 2007, Pocketbook on integrating HIV/AIDS considerations into food security and livelihoods projects,
112 Overseas Development Institute, 2010, High World Food Prices,
FAO, 2011, World Food Situation,
113 WHO, 2008, Regional Consultation on Nutrition and HIV/AIDS in French Speaking Countries in Africa Region,
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
Western Pacific region which focused on strengthening services and community involvement in order to tackle HIV/AIDS and under- and maln
2.3 Diseases and Co-infections
HIV/AIDS leaves a patient increasingly vulnerable to other diseases rather than having a direct effect
on the well-being of the patient. Consequently, all deaths attributed to AIDS are also strongly
associated with other diseases. Tuberculosis (TB) in particular, is the leading direct cause of death in
HIV/AIDS patients. The largest contributor to the spread of tuberculosis in Africa during the past two
decades has been HIV/AIDSand of the 9.4 million people infected with TB in 2008, an estimated 1.4
million were also infected with HIV. Approximately 520 000 patients die each year from TB (26% of
total HIV/AIDS deaths). The risk of contracting TB is estimated to be between 20-37 times greater for
HIV infected people than for the general
pAntiretroviral treatment of
Fig. 12: Overlaps between HIV and TB
HIV/AIDS reduces the risk of HIV-
(incidence and deaths)
associated tuberculosis by As part of their Global Health Sector Strategy
on HIV/AIDS, the WHO recommends the following target: "reduce tuberculosis deaths by 50% (compared with a 1990 Deathsbaseline)" by 2015 Not only does HIV/AIDS increase suscep-
tibility to tuberculosis, but tuberculosis
also speeds the progression of HIV into AIDSas does pneumonia, malaria, and
Sources: WHO et al. 2010 (fn. 45), pp. 50-73;
most other communicable dise
WHO 2011: World Health Statistics 2011, p. 16.
There is some debate over whether this is true for viral diseases such as measles, as some studies have indicated that while the measles virus is active, the replication of HIV is sloHowever, infecting HIV patients with measles is not recommended as a strategy to fight HIV/AIDS, since people with compromised immune systems are naturally more susceptible to This in turn has lead to concern over whether HIV/AIDS patients should receive the measles vaccine (an attenuated "live" vaccine). A 2009 systematic review and meta-analysis published by the WHO concluded that there is no increased risk in vaccinating HIV infected children with the measles vaccine. The same study also recommends that severely immunocompromised patients should not receive the vaccine. When CD4 cell counts are too low, the vaccine is usually ineffective, and therefore the risks do not outweigh the benefits in severely immunocompromised p(because attenuated vaccines rely on the creation of antibodies within the patients own body to create immunity). When vaccinating people living with HIV, administering antiretroviral therapy directly before a measles vaccination therefore helps promote the creation of antibodies, increasing the effectiveness of the va
114 UNICEF, 2010, Health, Nutrition, & HIV and AIDS
115 WHO, 2010, Tuberculosis, Fact Sheet No. 104 116 WHO et al. 2010 (fn. 45), pp. 50-73.
117 WHO, 2011, Antiretroviral therapy for HIV p.
118 WHO 2011 (fn. 59), § 22; resolution WHO 2011, 64th World Health Assembly: Draft global health sector strategy on HIV,
119 WHO et al. 2010 (fn. 45), pp. 50-73.
120 Hewitt, K. et al., 2006, Interactions between HIV and malaria in non-pregnant adults: evidence and implications. AIDS vol. 20
121 Garcia, M. et al., 2008, Measles virus inhibits human immunodeficiency virus, Journal of General Virology, Vol. 89,
122 WHO, 2009, WHO Weekly Epidemiological Record, No, p. 325-332. 123 Ibid.
124 Pensieroso, S., et al., 2009, Timing of HAART defines the integrity of memory B cells and the longevity of humoral responses
in HIV-1 vertically-infected children. In: Proceeding of the National Academy of Sciences
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
Other diseases are closely linked to HIV/AIDS via their transmission pathways. Blood safety is not only important for limiting the spread of HIV/AIDS, but also hepatitis B and C. HIV-infected people are also more susceptible to infection with viral hepatitis B Furthermore, HIV infection may reduce the protective effect of the hepatitis B vaA co-infection with HIV and hepatitis C may lead to an accelerated course of liver as well as accelerated progression of HIV into AIDS. HIV co-infections with hepatitis B or hepatitis C are an increasing issue in countries with a high occurrence of HIV infTherefore it is recommended to integrate interventions for the prevention, treatment and care of hepatitis B and C virus infections into existing HIV focused se Reproductive health and safety initiatives also integrate HIV/AIDS prevention and awareness measures with other sexually transmitted infections (STIs, including hepatitis B). Not only are these topics well suited to be addressed together, but, the presence of other STIs (both ulcerative and non-ulcerative) greatly increases the risk of acquiring or transmitting HIV/AIDS (by a factor of up
As well as being increasingly susceptible to existing diseases, immunocompromised individuals become increasingly susceptible to new diseases. Surveys in Latvia and the Ukraine found nearly twice the level of antibiotic-resistant TB among TB patients living with HIV compared with TB patients without HIV. Antiretroviral resistant HIV is also a serious concern, and the WHO has described its development as inevitable due to the fast replication and mutation rates of the HI virus, and the need for lifelong antiretroviral treatment of p Additionally, HIV/AIDS itself may mutate to a more virulent form, including the already emerging forms of drug resistant HIV strainsTherefore, clinics treating HIV/AIDS patients should be attentive to both the development of new diseases, as well as signs that the HI virus is increasing in virulence.
Indoor air pollution is another important health consideration for HIV/AIDS patients. HIV/AIDS patients are particularly vulnerable to respiratory problems, eye infections, and other problems associated with indoor air pollution such as the cooking smoke from open fires
2.4 Safe Injections and Sterile Medical Equipment
Unsterile medical equipment is an important vector for the transmission of HIV, and injection safety is a
particular concern. Contaminated injections result in about 8-20.6 million new cases of hepatitis B
infection, 1-4.7 million cases of hepatitis C infection, 3 million cases of bacteraemia, 850 000 cases of
injection site abscess and, more alarmingly, 80 000 to 340 000 cases of HIV infections per year
Making sure that injection equipment (as well as other surgical equipment) is sterile not only prevents the spread of HIV, but the spread of other diseases transmitted via blood or bodily fluids.
The UN established an internationally agreed upon goal of implementing universal precautions in health-care settings to prevent the transmission of HIV infection by Although this has not been fully achieved, HIV/AIDS infections caused by unsafe injections have been reduced by half between 2001 and
125 WHO 2002, Hepatitis B p. 7; WHO
2002a, Hep. 35.
126 WHO 2002 (fn. 125), pp. 50, 54.
127 WHO 2002a (fn. 125), p. 48.
128 WHO, 2010, Viral hepatitis; Report by the Secretariat. (A63/15) 2010,
129 Ibid., p. 15.
130 WHO, 2007, Fact sheet No. 110, Sexually Transmitted Infections
131 WHO, 2011, HIV drug resistance strategy 132 Ibid.
133 Deutsche Gesellschaft für Technische Zusammenarbeit (GTZ) GmbH, 2009: Mainstreaming HIV in the Energy Sector.
(Guidance for German Development Cooporation.) .
134 Hauri et al. [WHO], 2004 (fn. 6), p. 1831; Kane et al., 1999 (fn. 6), p. 803; SIGN/WHO, 2011 (fn. 9), p. 4.
135 Resolution of UN, 2001 (fn. 34).
136 SIGN/WHO, 2011 (fn. 9), p. 4.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
Precautions in Medical Environments Recommended by WHO
Communication of risks associated with unsafe injections to patients through disease prevention programmes (such as HIV prevention)
capacity building of all health care workers in best injection and related procedures and practices
the use of protective barriers
preventing two-handed recapping of needles
ensuring access to sufficient quantities and quality of injection equipment in health care facilities:
for therapeutic injections, either reuse and needle stick prevention syringes or single-use disposable injection equipment
for immunization injections, auto-disable syringes exclusively
covering all cuts and abrasions with waterproof dressings
prompt clean up of spills of blood or other bodily fluids
safe collection of medical waste and disposal of sharps to prevent the reuse of dirty equipment and needle-stick injuries (safety-boxes, syringes with needle-stick prevention feature)
Sources: WHO 2002 (fn. 6), pp. 130-131; Hauri et al. [WHO]
2004 (fn. 6), p. 1840; SIGN/WHO 2011 (fn. 9); AVERT, 2011 (fn. 8), p. 3: WHO 2009.
2.5 Occupational Safety
HIV/AIDS creates a large challenge to economic and social development and can endanger public
workplaces, as HIV/AIDS's highest concentration of victims are among adults of working age. The
workforce of over 30 countries may be between 10-35% smaller by 2020 due to HIV/AIDS Health care professionals, sex workers, and highly mobile labourers have a far greater risk of being
infected with HIV than the individuals of other professions. They are classified as "high-risk workers".
Health care professionals carry a high risk mainly due
Effects of HIV/AIDS on the Workforce
to their heightened exposure to blood and other bodily The primary source of transmission in
• Costs borne by employers can increase:
the medical field is through percutaneous infection
o productivity can decline and lead to (i. e. from needles, instruments and bites). Fortunate-
weakened economic development;
ly, the average rate of transmission after such an
o skilled workers may become scare
incident is only about 3 in 1
• overall labour force:
Since 2005 the HIV prevention efforts for high-risk
o absenteeism and early retirement individuals has tripled. These high-risk individuals
include sex workers, and out of the 39 countries that
o stigmatization and/or discrimination report to have HIV-prevention services for sex wor-
of HIV-positive employees;
kers, only a 60% average coverage rate
• food may become insecure as rural wor-
Within medical environments, health care workers
kers are among the highest concentration should follow the precautions that are advised by the
of the infected;
World Health Organization (see box above).
• increased poverty, due to the loss of the The workplace offers an excellent platform for
family 'breadwinner';
fighting the HI virus by educating workers and pro-
• an increased demand for public services viding practical prevention tools. Although education
and crucial supplies;
campaigns may be initially costly, inaction by
• distorted markets
companies can result in increased production costs
ILO (fn. 137), p. 13. due to heightened levels of HIV/AIDS and the
137 ILO, (no date), Factory Improvement Programme: HIV and AIDS in the Workplace, Training Guide
138 AVERT, 2011 (fn. 8).
139 WHO, 2010, HIV/AIDS: Online Q140 UNAIDS, 2008, Press Release: Substantial Increases in HIV Prevention Efforts Producing Results, but not Enough to Turn Back
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
associated productivity losses (researchers from the Center for International Health at Boston Uni-versity found that new infections can cost employers between 3.4% and 10.7% of annual salaries, dependent on skill level, associated benefits, etc.The ILO recommends measures focusing on the prevention and management of the impact of HIV/AIDS in the workplace, care and support for infected workers, and the elimination of discrimination and stigmatization on the basis of a real or assumed HIV status
2.6 Gender Equity
The proportion of women living with HIV/AIDS has remained stable at slightly less than 52%
worldwidWomen face double the risk of contracting HIV than men during sexual intercourse with
an infected partner. Statistically, women also tend to be infected earlier in life. Power imbalances often
limit women's capacity to negotiate safer sex, as many men do not respect the wants and needs of
their partners regarding safer behaviours. An unknown proportion of women have also become infected
with HIV through rape, which is linked to a threefold increase in the risk of HIV transmission. Addition-
ally, many women are economically forced to work in the sex industry, which increases their risk of HIV
infWith antenatal and perinatal care and injectable birth control, women undergo a higher
proportion of injections and, accordingly, a higher risk of HIV inf Many cultures hold gender-related beliefs that prevent women from taking the necessary steps to
protect themselves from HIV transmission. For example, in certain cultures it is considered in-
appropriate for a woman to initiate the frank, assertive discussions about sex and disease risk that are
necessary to implement preventative measures (such as condom use)In other instances, the
emergence of HIV/AIDS has lead to an increase in practices that violate women's rights, such as
certain forms of virginity In other instances cultural myths have lead directly to rape, such as
the belief that sex with a virgin can protect one from HIV/AIDSor even heal an already infected
pe
2.7 Safe Birthing Conditions
There are 2.5 million children living with and another 10 000 become infected each dayFurthermore, an estimated 260 000 children under the age of 15 died of AIDS related illnesses in
Children are usually infected by their HIV-positive mothers during pregnancy, delivery, breast-
feeding or by unsafe injections in perinatal and pediatric health care.
141 ILO, 2002, Good Practice Note HIV/AIDS in the Workplace
142 ILO, 2001, An ILO Code of Practice on HIV/AIDS and the World of Work
143 UNAIDS 2010 (fn. 1), p. 23.
144 UNAIDS 2010 (fn. 1), pp. 10-11, 130-136; UNAIDS 2010a, Joint United Nations Programme on HIV/AIDS: Fact Sheet 10:
Women, Girls and HIV. 1 March 2010
Action Aid 2008, Hit or miss? Women's rights and the Millennium Development Goals. London,
145 Reid, S., 2010, Preliminary results of the update of the WHO global burden of disease from unsafe medical injections.
Presentation at the 11th annual meeting of the Safe Injection Global Network (SIGN/WHO), 9 November 2010, Dubai, p. 8.
146 Levinson, R. A., et al., 2004, The impact of cultural context on Brazilian adolescents' sexual practices,
, pp. 217-221.
147 Leclerc-Madlala, S., 2001, Virginity Testing: Managing Sexuality in a Maturing HIV/AIDS Epidemic, Medical Anthropology
Quarterly 15 (4) , pp. 533-552.
148 Motzoi, C., 2006, Combating HIV/AIDS: Promoting Gender Equality among Youth, World Bank, Washington, DC
149 Meel, B., 2003, The Myth of Child Rape as a Cure for HIV/AIDS in Transkei: A Case Report, Medicine, Science and the Law
150 UNAIDS 2010 (fn. 1), p. 182.
151 Ibid., pp. 19, 78, own calculation.
152 Ibid., p. 19.

HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
Around half of the infants born to HIV-positive mothers are pre- or perinatally infected with HIV, which contributes to 90% of all childhood HIV infAlthough most infants are not infected during pregnancy, the process of delivery and the associated breaking of membranes may cause the HI virus to spread to the child. In order to reduce this risk, a caesarean section may be recommended. Traditionally, this is most often the case for women who are not taking any ARV treatment, because for women who are, the rate of transmission is already reduced, and the risks of surgery in low and middle income countries can often outweigh the benefits. These risks include haemorrhage, post-postpartum fever, wound infection and sepsis. The WHO recommends that the safety of surgery should be impro-ved as a part of the fight against the HIV/AIDS Elective caesarean sections decrease the risk of transmitting HIV by 50% (the transmission rate for women who underwent elective caesarean
section was 8.4%, compared to 16.7% for those who did not). Furthermore, for women receiving ARV treatment, an elective caesarean section decreased the transmission rate from 7.3% to 2% (which equals a reduction of transmission risk by Another stage of development at which of mother-child transmission occurs is during breastfeeding. Despite this risk of transmission, breastfeeding by HIV-positive women is often less dangerous than formula feeding because of the life-threatening diseases present in unsafe water, and the immu-nity that is transmitted through breastmilk. The likelihood of transmission can be significantly lowered (by 42-54%) if the mothers receive ARV treTherefore, ARV treatment is of paramount importance for mothers who have no alternative to breastfAnother option would be to provide equip-ment to heat breastmilk. The rates of perinatal and breast-feeding transmission have been decreasing; from 500 000 in 2001 to about 370 000 in 2009albeit at about half of the
Kaka woman with her youngest brother, targeted 50% r
See section 1.8 on measures on this issue
The latest documented stage at which caregiver to child transmission occurs is during the pre-mastication of food for infants (when an adult chews food before feeding it to the infant). Infection occours when blood from an infected caregiver's mouth mixes with the food while chewing. Pre-mastication of food for children is common in many parts of the wo
One of the predominant obstructions to further reducing mother-child transmission rates is insufficient access to antenatal and postnatal care. With adequate access to services, mother-child transmission can often be prevented. An antiretroviral (ARV) regimen is recommended during the pregnancy, delivery and breastfeeding stages of development. Recently a triple ARV regimen was shown to decrease HIV infections in newborns by 42-54% compared with the control ARV rIn addition to ARV regimens, more inclusive antenatal and postnatal care should include voluntary testing, prophylactic treatment, and optimal obstetric care. Despite these relatively simple preventative solutions, many women in the developing world do not have any access to these services and others
153 UK Center for disease Control and Prevention, 2011, 19994-GP Notebook: UK Medical Reference,
154 WHO 2011 (fn. 59), §§ 36 and 67.
155 Northwest AIDS Education and Training Center/University of Washington, 2011, Perinatal Discussion, own calculation
156 Kesho Bora, 2011 (fn. 55), pp. 6-8; WHO, 2011, Kesho Bora Study: Preventing mother-to-child transmission of HIV during
breastfeeding, Polic, p. 2.
157 WHO et al., 2008 (fn. 43), pp. 35, 37-38; WHO, 2010 (fn. 45), p. 79.
158 WHO, 2010 (fn. 45), pp. 19, 78. 159 Ibid., p. 64.
160 Gaur, A. H., et al., Practice of Feeding Premasticated Food to Infants: A Potential Risk Factor for HIV Transmission. Pediatrics.
2009, 124:658-666p. 66.
161 Kesho Bora (fn. 55), 2011, p. 1.

HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
may have only partial access. In 2009, only 26% of pregnant women had access to HIV tNevertheless, there has been an increase in the amount of confirmed HIV-positive, pregnant women in low and middle income countries receiving antiretroviral medication to prevent mother-child trans-mission, from 15% in 2005 to more than 60% in Continuing and strengthening education on HIV/AIDS prevention, obstetric care, and AVR treatments for HIV-positive mothers and mothers-to-be will continue this trend.
2.8 Access to Safe Water and Sanitary Living Conditions
Although HIV/AIDS is not directly a water-related disease,
access to safe water and sanitary living conditions can
improve the health of those already living with HIV/AIDS,
relieve the burden of caregivers, and preserve human
dignityThe majority of opportunistic infections, which are
the primary direct killers of HIV/AIDS sufferers, are often
transmitted via contaminated water and unsanitary living
conditionIn addition, diarrhoea, a common symptom of
the aforementioned infections, can be deadly without access
to clean water for re-hydration. Large amounts of clean water
as well as hygienic latrines are necessary to protect the
individual from waterborne diseases and prevent further
Women washing their laundry, India
contamination of the community. If there is no access to clean water, HIV-positive mothers tend to breastfeed their children even if they are aware of the risk of HIV transmis
2.9 Environment, Consumption of Natural Resources, and Land Usage
Natural resources serve as a "safety net" for households unable to maintain their livelihood as a result of HIV/AIDS and or povertySince natural resource collection is, in general, less labour-intensive and requires little to no start-up capital, HIV/AIDS affected communities often become more heavily reliant on the natural resources available to This increased dependence on natural resources has anecdotally been linked to a decline in their prevalence, quality, predictability, and/or accessibilityReciprocally,
Members of women's council, with
medicines col ected from the fields, Nigeria
162 WHO et al. 2010 (fn. 45), 86; UNAIDS 2010 (fn. 1), p. 78; AVERT, 2011 (fn. 8), p. 3.
163 UNAIDS 2011 (fn. 54), p. 72; WHO et al. 2010 (fn. 45), pp. 78, 83.
164 World Bank, 2011, Water and Sanitation Program: Access to Water Supply and Sanitation Improves Quality of Life for People
166 IRC (International Water and Sanitation Centre), 2007, HIV/AIDS and Water, Sanitation and Hygiene
167 Bolton, S., and Talman, A., 2008, Centre for Disease Control and Prevention, Male Circumcision and Risk for HIV Transmission
and Other Health Conditions: Implications for the United States,
Feldbaum, H., et al., 2006, The National Security Implications of HIV/AIDS, Public Library of Science
168 Bolton, Talman, 2008 (fn. 167).
169 Challe, J. F., and Price, L. L., 2009, Endangered edible orchid and vulnerable gatherers in the context of HIV/AIDS in the
Souther Highlands of Tanzania, Journal of Ethnobiology and Ethnomedicine, Vol. 5.
Dwasi, J., 2002, HIV/AIDS and Natural Resource Management in Africa: Findings from Kenya, Namibia., South Africa and Uganda (Draft).
Mauambeta, D. D. C., 2003, HIV/AIDS Mainstreaming in Conservation: The Case of Wildlife
and Environmental Society of Malaw
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
shortages in natural resources reduce peoples coping ability, thereby leading to increased vulnerability to poverty, and therefore also to HIV/AIDS HIV/AIDS also causes changes in land usage. Rural communities burdened by HIV/AIDS often experience a decreased availability of labour and land management capacity, and a loss of indigenous knowledge on resource management and biodiversity conservDr. Marcela Vilarreal, a Senior Officer for the UN Food and Agriculture Organization (FAO) of the United Nations' Sustainable Development department explained the problem in the following terms: "Innovation often dies with the
farmers . They have developed ways to adapt their crops to the environment and when they die, so
does their knowledge. Biodiversity is also threatened because in times of acute labour shortages,
people plant fewer varieties of crops to save time and
Women and children washing clothes and softening maize in a stream, Nigeria
2.10 Conflict, Human Rights, and International Security
Many factors that make manage-
"The threats to peace and security in the twenty-first century
ment and treatment of HIV/AIDS
include not just international war and conflict but civil violence,
difficult are magnified by con-
organized crime, terrorism and weapons of mass destruction.
For example sexual vio-
They also include poverty, deadly infectious disease and envi-
lence, high risk behaviours, isola-
ronmental degradation since these can have equally catastro-
tion and insecurity of affected re-
phic consequences. All of these threats can cause death or
gions complicate the delivery of
lessen life chances on a large scale. All of them can undermine
supplies and equipment, and leads
States as the basic unit of the international system.
to the breakdown of social and
In our globalized world, the threats we face are interconnected
healthcare infrastructure. Personal
. On this interconnectedness of threats we must found a new
trauma and the death of key sup-
security consensus, the first article of which must be that all
port leaders may decrease general
are entitled to freedom from fear, and that whatever threatens
willingness to be treated, and (al-
one threatens all. Once we understand this, we have no choice
though against international
but to tackle the whole range of threats. We must respond to
humanitarian law) targeting of aid
HIV/AIDS as robustly as we do to terrorism and to poverty as
workers can lead to a lack of
effectively as we do to proliferation. We must strive just as
qualified staffAlthough the
hard to eliminate the threat of small arms and light weapons as
magnification of these factors may
we do to eliminate the threat of weapons of mass destruction.
contribute to a possible increase
Moreover, we must address all these threats preventively,
in HIV transmission in conflict-
acting at a sufficiently early stage with the full range of avail-
ridden arit is still unclear
able instruments."
whether such vulnerability neces-sarily translates to an increased
Kofi Annan, 2005, In Larger Freedom, §§ 78-81 .
rate of transmission, as each
170 IUCN, 2010, HIV/AIDS and the environment: A review of Evidence and Recomendations for Next Steps
171 Bolton, Talman, 2008 (fn. 167); Torella, E., et al., 2006, Ocean & Coastal Management, Examining the linkages between AIDS
and biodiversity conservation in coastal Tanzani, 49(11), 792-811.
172 Vilarreal, [in] FAO, 2001, Indigenous knowledge - a key weapon in fighting HIV/AIDS
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
conflict presents different factors contributing to either an decrease or increase of transmission, making it difficult to claim that conflict has a direct effect in HIV transmissionsIn fact it is possible that areas affected by long conflicts, even when with sexual violence is an issue, may have a low HIV-infected population in comparison to host countries without such conflicts. For example, the eastern Democratic Republic of Congo showed an increase in HIV transmission due to sexual violence perpetrated by paramilitary and foreign military personnel on the local population, while Sierra Leone, Southern Sudan and Angola did not. This may be due to the nature of isolation of refugee population and internally displace peoples (Iwhich, contrary to popular belief, often have a lower HIV-infected rate than the surrounding host Despite this, stigmatization of refugees and IDPs is still an issue. This is especially true for women and girls who have been raped as a "weapon of war" by host states, members of their society or in their state of origin. This leaves these vulnerable populations to face an already high rate of human rights abusesFurthermore, either a real or per-ceived lack of confidentiality, discrimination, denial of access to asylum procedures, threats of refoulement or restrictions of freedom and other consequences have been proven to make people living with HIV/AIDS reluctant to seek treatmeTherefore, strict standards of confidenti-ality and equal opportunity should be in place in conflict-ridden areas in order to minimize the spread of HIV/AIDS. Additionally, because of the frequency of human rights violations in areas of conflict, the UNHCR (United Nations High Commissioner for Refugees) recommends the fol-
Discarded bomb casings, Laos
• "No denial of access to asylum procedures, refoulement or denial of right to return on the basis of
• No mandatory HIV testing of displaced persons under any circumstances.
• When required by countries in which refugees have requested resettlement, HIV testing conducted
in accordance with established standards (i. e., accompanied by pre- and post-test counselling and
appropriate referral for follow-up support and services).
• Effective procedures in place to maintain confidentiality of individuals HIV status.
• Informed consent by clients for disclosure of their HIV status if such disclosure is necessary to
obtain community or protection services.
• Policies, laws and programmes in place to combat stigma and discrimination against people living
with HIV/AIDS.
• No laws or regulations prohibiting displaced persons access to public sector HIV/AIDS program-
173 IFRC, 2008 (fn. 98).
174 Ibid.
175 International Committee of the Red Cross (ICRC), 2008: HIV/AIDS field guide; A planning and practice guide to integrating
HIV/AIDS into the ICRC's health p. 6.
176 Spiegel, P., 2004, HIV/AIDS among conflict-affected and displaced populations: dispelling myths and taking action, Disasters,
Vol. 28, Nopp. 322-339.
177 Mock, N., et al., Conflict and HIV: A framework for risk assessment to prevent HIV in conflict-affected settings in Africa,
Emerging Themes in Epidemeology, vol. , p. 6.
178 IFRC, 2008 (fn. 98).
179 Ibid.
180 Spiegel, 2004 (fn. 176).
181 Spiegel, 2004 (fn. 176), p. 331.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
2.11 Preparedness for Natural Disasters
The social and economic upheaval resulting from disasters potentially increases risk-taking, sexual and
gender-based violence (including rape) and other behaviours which are linked to an increase in
HIV/AIDS (including forcing women whose livelihoods have been disrupted to work in the sex
Natural disasters may break family ties and alter sexual networking, which in turn
facilitates the spread of HIV/AIDSThe interruption of treatment and care regimes, the prevalence of opportunistic infections, unavailability of medical interventions to prevent mother-child transmission of the virus (antiretrovirals and caesarean sections where needed), limited availability of condoms and other preventative tools, and the lack of priority that reproductive healthcare and information services take on in an emergency situationThis can have serious consequences. For example, interruptions in an antiretroviral treatment regime can increase the development of an antiretroviral resistant HIV strainThese interruptions can be as a result of either the unavailability of antiretroviral drugs themselves, or the poor compliance that is associated with the increased side effects of antiretroviral drugs without adequate nutrition
Key Points
HIV/AIDS is responsible for 1.8 million deaths and 58.5 million lost healthy life-years (DALYS) each year.
People from every country are infected, but the most affected countries are also some of the poorest in the world.
HIV/AIDS is a global issue, with wide-reaching economic, political, social and environmental consequences, even for countries which do not have a high rate of infection.
Poverty, including the lack of access to food, antenatal health care and safe water, may be the strongest hurdle to fight the spread of HIV/AIDS and to reduce its human impact.
Many factors influence HIV/AIDS, and measures taken to fight it need to be undertaken with an understanding of the holistic global context of the epidemic for the measures to be most effective.
182 Oxfam, 2005, The Tsunami's Impact on Women, Oxfam Briefing Note
IFRC, 2008 (fn. 98).
183 IFRC, 2008 (fn. 98), p. 148.
184 Ibid., p. 144.
185 WHO 2010, HIV/AIDS; Online Q&A, July 2010, Bennett/Assefi 2005 (fn.
38), pp. 72-81; Bertozzi et al. 2006 (fn. 11), p. 358.
186 Ivers et al. 2009 (fn. 106), p. 1097; Bertozzi et al. 2006 (fn. 11), p. 352.
HIV/AIDS in the Context of Other Global Challenges
Special Report for the UN High-Level Meeting on AIDS
Goals
"Commit ourselves to addressing the rising rates of HIV infection among young people to ensure an HIV-free
future generation through the implementation of comprehensive, evidence-based prevention strategies,
responsible sexual behaviour, including the use of condoms, evidence- and skil s-based, youth-specific HIV education, mass media interventions and the provision of youth-friendly health services" "Intensify proven, cost-effective actions against diseases and malnutrition that are the major causes of child mortality and morbidity, including . reducing the incidence of . HIV/AIDS.
"By 2003, implement universal precautions in health-care settings to prevent transmission of HIV infection"
Targets
"Governments, with assistance from UNAIDS and donors, should, by 2005, ensure that at least 90 per cent, and
by 2010 at least 95 per cent, of young men and women aged 15 to 24 have access to the information, education
and services necessary to develop the life skil s required to reduce their vulnerability to HIV infection. Services
should include access to preventive methods such as female and male condoms, voluntary testing, counsel ing and fol ow-up. Governments should use, as a benchmark indicator, HIV infection rates in persons 15 to 24 years of age, with the goal of ensuring that by 2005 prevalence in this age group is reduced global y, and by 25 per cent in the most affected countries, and that by 2010 prevalence in this age group is reduced global y by 25 per
"By 2005, reduce the proportion of infants infected with HIV by 20 per cent, and by 50 per cent by 2010, by
ensuring that 80 per cent of pregnant women accessing antenatal care have information, counsel ing and other HIV-prevention services available to them, increasing the availability of and providing access for HIV-infected women and babies to effective treatment to reduce mother-to-child transmission of HIV, as wel as through effective interventions for HIV-infected women, including voluntary and confidential counsel ing and testing, access to treatment, especial y anti-retroviral therapy and, where appropriate, breast-milk substitutes and the provision of a continuum of care"
Human Rights
"The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human
being without distinction of race, religion, political belief, economic or social condition. "Everyone has the right to a standard of living adequate for the health and wel -being of himself and of his
family, including . medical care" The state parties of the International Covenant on Economic, Social and Cultural Rights „recognize the right of
everyone to the enjoyment of the highest attainable standard of physical and mental health. The steps to be
taken by the States Parties to the present Covenant to achieve the ful realization of this right shal include those necessary for: .
(c) The prevention, treatment and control of epidemic, endemic, occupational and other diseases;(d) The creation of conditions which would assure to al medical service and medical attention in the event of sickness The UN General Assembly "Recognizes that access to medication in the context of pandemics such as HIV/AIDS,
tuberculosis and malaria is one fundamental element for achieving progressively the ful realization of the right of everyone to the enjoyment of the highest attainable standard of physical and mental health" "Reaffirm that the ful realization of al human rights and fundamental freedoms for al is an essential element in the global response to the HIV/AIDS pandemic, including in the areas of prevention, treatment, care and support,
and recognize that addressing stigma and discrimination is also a critical element in combating the global
HIV/AIDS pandemic"
187 Resolution UN 2006 (fn. 65), § 26, emphasis added.
188 Resolution UN 2002 (fn. 34), § 37 (11), emphasis added.
189 Resolution UN 2001 (fn. 34), § 51.
190 UN 1999, § 70, emphasis added; similar: resolutions UN 2001 (fn. 34), § 47, and UN 2002 (fn. 34), § 46.
191 Resolution UN 2001 (fn. 34), § 54, emphasis added, and UN 2002 (fn. 34), § 46.
192 WHO 1946 – World Health Organization: WHO Constitution193 UN 1948: Universal Declaration of Human Ri, Article 25.1.
194 UN 1976: International Covenant on Economic, Social and Cultural Righ, art.
12, emphasis added.
195 UN 2004: Resolution adopted by the General Assembly 58/179, Access to medication in the context of pandemics such as
HIV/AIDS, tuberculosis and malari, emphasis added.
196 Resolution UN 2006 (fn. 65), emphasis added.
Source: http://global2015.de/file/global2015hiv.pdf
DORAMECTINA 1,1%. Endectocida altamente efectivo para el control y tratamiento de los parásitos internos y externos. NOVIEMBRE DE 2013 Doramectina es una lactona macrocíclica Figura 1. Origen y clasificación de las lactonas semisintética, perteneciente a la familia de macrocíclicas: avermectinas y milbemicinas (tomado de Lifschitz y col 2002).
CRCP/ DCS 9:201X DRAFT NO. 3 CARICOM REGIONAL CODE OF PRACTICE Code of practice for organically produced foods DCS/ CRCP 9:201X Caricom Regional Organisation for Standards and Quality, CROSQ 2ND Floor Nicholas House 29 & 30 Broad Street Bridgetown, St Michael Barbados Telephone: 246-622-7677 Fax: 246-622-6778 Email: [email protected] Website: http://www.crosq.org