Microsoft word - 5_dr. chaitanya tingane_choking_ case report.docx
Vol 23, Number 1 Journal of Forensic Medicine, Science and Law
(Jan-Jun 2014) A Journal of Medicolegal Association of Maharashtra
Case Report
DEATHS DUE TO CHOKING AMONG PSYCHIATRIC PATIENTS
A REPORT OF THREE CASES
Dr. CV Tingne, Dr. NB Kumar, Dr. PS Ghormade, Dr. RK Gadhari, Dr. AN Keoliya
Dr. Chaitanya Vidyadhar Tingne Assistant Professor, Department of Forensic Medicine & Toxicology, Indira Gandhi Government Medical College, Nagpur, Maharashtra, India (440018) Dr. Narendra Baluram Kumar Assistant Professor, Department of Forensic Medicine & Toxicology, Indira Gandhi Government Medical College, Nagpur, Maharashtra, India (440018)
Dr. Pankaj Suresh Ghormade Assistant Professor, Department of Forensic Medicine & Toxicology, Indira Gandhi Government Medical College, Nagpur, Maharashtra, India (440018)
Dr. Ramesh Kashinath Gadhari Assistant Professor, Department of Forensic Medicine & Toxicology, SBH Government Medical College, Dhule, Maharashtra, India Dr. Ajay Narmadaprasad Keoliya Professor and Head, Department of Forensic Medicine & Toxicology, Indira Gandhi Government Medical College, Nagpur, Maharashtra, India (440018) Number of Pages:
Number of Tables:
Number of Graph:
Number of Photographs:
Corresponding Author:
Dr. Chaitanya V. Tingne
First floor, Plot no. 70,
West High Court Road, Bajaj Nagar,
Nagpur, Maharashtra, India, 440010
[email protected], 9822864460
Vol 23, Number 1 Journal of Forensic Medicine, Science and Law
(Jan-Jun 2014) A Journal of Medicolegal Association of Maharashtra
Case Report
DEATHS DUE TO CHOKING AMONG PSYCHIATRIC PATIENTS
A REPORT OF THREE CASES
Dr. CV Tingne, Dr. NB Kumar, Dr. PS Ghormade, Dr. RK Gadhari, Dr. AN Keoliya
Abstract
Choking is a form of asphyxia caused by an obstruction within the air passages most
commonly by a food bolus lodging in the larynx or laryngopharynx. Choking incidents have
long been recognized as a cause of death in people with mental illness and is one of the
mechanisms postulated to connect the use of antipsychotic medication with sudden death.
Choking deaths, if observed, are sudden and dramatic, and their common association with
active eating is such that a report of the death is made to the authorities. We present here a
report comprising of three psychiatric patients who died of accidental choking while eating.
Key words: Choking, psychiatric, atypical antipsychotics
Introduction
Choking is a form of asphyxia caused by an obstruction within the air passages most
commonly by a food bolus lodging in the larynx or laryngopharynx. A large foreign body
may be impacted in the pharynx and cause death from hypoxia. A small object partially
blocking the lumen of the larynx may cause death by laryngeal spasm. Irritation of tracheal
mucosa by foreign body may cause death by reflex parasympathetic cardiac inhibition.
Patients with serious mental illness, especially those who are elderly, have poor dentition and
eating habits, or take antipsychotics with anticholinergic and/or dopamine blocking effects,
are at an increased risk of death due to choking. Choking incidents have long been recognized
as a cause of death in people with mental illness and is one of the mechanisms postulated to
connect the use of antipsychotic medication with sudden death [1]. In addition to psychiatric
patients; groups with higher choking risk include young children, the elderly, especially those
with dementia, learning disabilities, intellectual disabilities and neurological patients. Some
of them share the similar problem of imperfect mental status. In India the law mandates
reporting to the authorities of any death that has occurred while mentally ill patients are held
involuntarily in the care of a mental health service. Choking deaths, if observed, are sudden
and dramatic, and their common association with active eating is such that a report of the
death is made to the authorities. We present here a case report comprising of three psychiatric
patients who died of accidental choking while eating.
Case report 1
A dead body of 68 year old female was brought for medicolegal postmortem
examination. The deceased was mentally ill, undergoing treatment at Regional Mental Hospital. The total daily doses for the psychoactive medication regimen included Risperidone 2 mg daily for psychosis and mood lability and Clozapine 500 mg for mood lability. As per history narrated by the hospital staff, she had bouts of coughing and respiratory distress while she was taking food. She collapsed on the floor and in spite of prompt resuscitative measures could not be revived and declared dead.
Externally, the subject was averagely built; postmortem staining was present and
fixed over the back and dependant parts of the body. There was bluish discoloration of finger and toe nails and lips. There were no external injuries seen. Internally all viscera were

Vol 23, Number 1 Journal of Forensic Medicine, Science and Law
(Jan-Jun 2014) A Journal of Medicolegal Association of Maharashtra
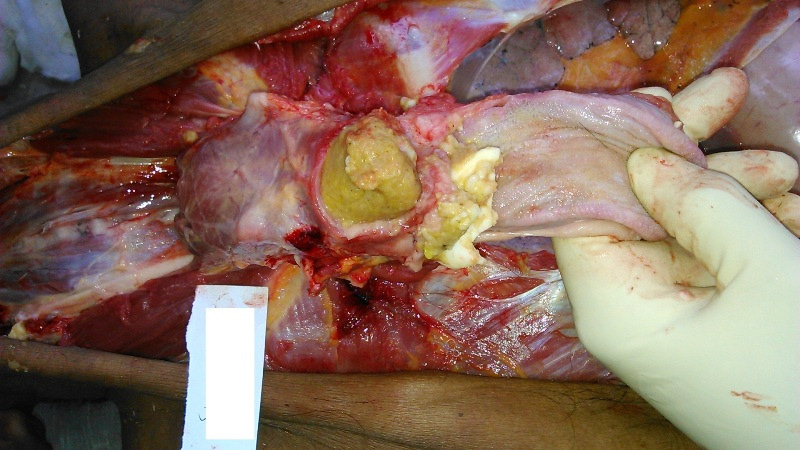
congested. Stomach contained undigested food particles. Identical food bolus was present in
larynx completely occupying the lumen (figure 1) with blood stained froth in trachea. Lungs
were oedematous exuding dark red color bloody fluid.
preserved and sent for chemical
common poisons and any sedative drugs. Viscera were
histopathological examination to rule out other pathologies. Both the
Fig 1: Food bolus completely occluding the laryngeal opening
cause of death was due to
asphyxia due to choking. Circumstances were consistent with accidental choking.
Case report 2
A 62 years old female corpse was brought for
autopsy to the mortuary. She had a 22 year history of paranoid schizophrenia and was being treated with Olanzapine for many years. Two weeks ago, she had stopped taking her medication and was brought to a State run psychiatric hospital because of worsening paranoia and hostility. She was a known case of type II diabetes and poor dentition. She has no history of substance abuse. Just before her death, a few minutes after beginning her meal, she suddenly stood up and put her hands to her throat. She looked frightened, was not able to speak and became unconscious. She was then taken to the emergency department, where she was declared dead.
On external examination she was well built and
nourished weighing 81 kg. There were no external injuries. Cyanosis was evident over fingernail beds and palms. Internally all organs were congested. A white colored partially chewed piece of cottage cheese was found occluding the laryngeal lumen (figure 2). Trachea contained semisolid food particles. Identical undigested food particles were present in stomach. Histopathological examination of organs and chemical analysis of viscera were non significant. The cause of death was respiratory
and cardiac failure secondary to choking and foreign
Fig 2: Piece of cottage cheese in
body obstruction.
infra glottic region
Case report 3:
A corpse of 75 year old male was brought for medicolegal postmortem examination
with an alleged history of sudden death while having breakfast. The deceased had a 40 year
Vol 23, Number 1 Journal of Forensic Medicine, Science and Law
(Jan-Jun 2014) A Journal of Medicolegal Association of Maharashtra
history of paranoid schizophrenia, which has been well controlled with Olanzapine, 20 mg/d,
for many years. He was a known case of hypertension and ischaemic heart disease and was
undergoing treatment at Regional Mental Hospital since four decades. The deceased while
eating breakfast abruptly stood up and put his hand against his throat and collapsed. In spite
of resuscitative measures he died within an hour of the onset of symptoms.
At autopsy on external
examination the deceased was a thin built male weighing 47 kg. Pieces of partially chewed up bread were present in the oral cavity.
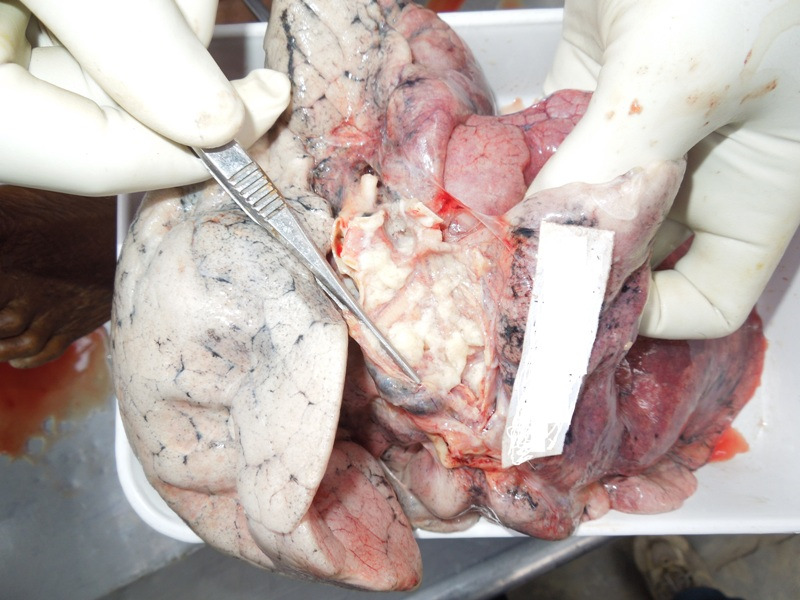
revealed brown colored piece of bread occluding the lumen of larynx. Whitish semisolid food particles mixed with mucus were present in the trachea and right principal bronchus (figure 3). Stomach contained undigested food material identical to that
found in trachea and larynx.
Fig 3: Aspirated food material in the right main bronchus Signs suggestive of asphyxia
Routine viscera chemical analysis and histopathological examination of organs failed to
reveal any associated pathology. The cause of death was asphyxia due to choking.
Discussion
Death from choking can be the result of pure hypoxia from occlusion of the airway,
when all the attendant signs of congestion, cyanosis and perhaps petechiae may be present, usually where the victim struggles to breathe for an appreciable period. However a large proportion of deaths occur suddenly before any possible hypoxic manifestations have time to take effect; these fatalities must be caused by neurogenic cardiac arrest, either purely neurogenic or accelerated by excess catecholamine release from the adrenaline response [2].
Reports on serious impairment of swallowing mechanism attributable to the side
effects of psychotropic drugs appeared in literature soon after the introduction of phenothiazines [3]. Psychiatric and geriatric patients often tend to have difficulty swallowing food particles, thus predisposing them to choking and aspiration [4]. The high incidence of tachyphagia among patients with schizophrenia has been noted, as has the frequent abnormality of such patients' swallowing mechanisms. This could predispose individuals with schizophrenia to choking [5].
All the three patients in the case report were elderly and were on atypical
antipsychotics. Some authors have pointed out how the well-known depression of the bulbar centers, variously brought about by all kinds of psychotropic medication, causes, among other things, an inhibition of the cough reflex, the swallow reflex, and the gag reflex. Moreover, patients on psychotropic drugs may theoretically have a combination of: 1) dopaminergic blockade with peripheral and central effects on deglutition (block or timing upsets in the components involved in the swallowing process) and 2) cholinergic blockade with potential impairment of esophagus motility and the gag reflex.
Neuroleptics, antidepressants, and antiparkinsonians are often used together and have
an anticholinergic synergetic effect on the swallowing process. However, no direct, clear-cut
Vol 23, Number 1 Journal of Forensic Medicine, Science and Law
(Jan-Jun 2014) A Journal of Medicolegal Association of Maharashtra
connection has ever been shown between psychotropic drugs and fatal asphyxiation. Clinical
experience, single case reports, epidemiological surveys, and pathophysiology studies,
however, do suggest that they may play a key role through diverse pathogenetic mechanisms
[6].
Psychotropic medications sometimes increase appetite or food craving through an
effect on hypothalamus, through leptin and ghrelin metabolism. Some elderly patients, chronic schizophrenic and mentally retarded patients had poor dental health that might further impair the quality of food boluses to be swallowed [7].
Patients on psychotropic medications should be reviewed regularly for side-effects,
notably extrapyramidal and anticholinergic side-effects. Patients should be advised to eat
slowly if they have a problem with overeating and tachyphagia. Relatives should be alerted to
the possible choking risk in high-risk patients, and advised to feed those in their care slowly
with appropriate types and amounts of food. Nursing staff should be trained to identify
patients at high risk of choking and provide appropriate resuscitation measures if such
incidents occur. Analyses of choking incidents and regular audit can help to monitor trends
and implement effective risk management measures.
References
1. Hollister LE. Unexpected asphyxial deaths and tranquilizing drugs. AJ Psychiatry.
1957;114,1035-1038.
2. Burns A, Horan M, Clague J, McLean G. Geriatric Medicine for Old Age Psychiatrists.
Taylor and Francis, London New York 2006; 193-196.
3. Von Brauchitsch H, May W. Deaths from aspiration and asphyxia in a mental hospital.
Arch of Gen Psych. 1968; 18,129-136.
4. Simpson GM, Davis JM, Jefferson JW. Sudden Death in Psychiatric Patients: The Role of
Neuroleptic Drugs. American Psychiatric Association Task Force Report; 1987 27. Washington,DC: APA.
5. Saukko P, Knight B. Suffocation and asphyxia. In Saukko P, Knight B eds. Knight's
Forensic Pathology. 3rd ed. London. Hodder Arnold. 2004;pp- 352-365.
6. Fioritti A, Giaccotto L, Melega V. Choking Incidents among Psychiatric Patients:
Retrospective Analysis of Thirty-one Cases from the West Bologna Psychiatric Wards. Can J Psychiatry, June 1997, 515-520.
7. PHW Yim, CSY Chong. Choking in Psychiatric Patients: Associations and Outcomes.
Hong Kong J Psychiatry 2009;19:145-149.
Source: http://www.mlam.in/pdf/currentissue/06-dr.chaitanya-tingane-choking-case-report.pdf
BELIEVE MIDWIFERY SERVICES, LLC VULVAR DERMATOLOGIC CONDITIONS EFFECTIVE DATE: May, 2009 POLICY STATEMENT Certified Nurse Midwives and other clinicians who provide primary gynecologic care are likely to see women with lichen sclerosus and lichen simplex chronicus, and, while lichen planus is less common, early recognition is important.
MINISTERIO DE SALUD MINISTERIO DE SALUD Y DEPORTES PROGRAMA NACIONAL DE SALUD RENAL Dirección: Plaza del Estudiante s/n Teléfono: (2) 2495053 La Paz, Bolivia. Deposito Legal Nº 200 ejemplares Noviembre, 2005 MINISTERIO DE SALUD Y DEPORTES LA PAZ – BOLIVIA PARTICIPANTES EN LA ELABORACIÓN Y REVISIÓN DEL DOCUMENTO